ARSENIC EXPOSURE- CARCINOGEN
CONTENT:
- ARSENIC ESTABLISHED CARCINOGEN
- HEALTH PROBLEMS
- HEALTH EFFECTS - RESEARCHES
- TOXICOLOGICAL STUDIES
- Arsenic poses stroke risk
- Arsenic Contamination in Rice(IRRI) growing Countries
- Inner Mongolian
- Nepal
- Sri Lanka
- The largest mass poisoning, Bngladesh/India
- Arsenicosis In Bangladesh : Samta
- Reported 100,000 cases of arsenic skin lesions: Bangladesh faces outbreaks of cancer (WHO)
- Arsenic warning on 'sacred' water
-NEW- Exposure to arsenic could double risk of pneumonia in children under 5 years
-NEW- Differences between West Bengal and Bangladesh
- Related Topics
ARSENIC ESTABLISHED CARCINOGEN
Background
In the face of the heavily polluted surface water, the Indian and Bangladeshi governments and foreign aid agencies took action in the 1970s and ‘80s in order to provide the masses with safe water. These governments and agencies dug over a million public pipewells to shallow aquifers, providing the population with water that was believed to be clean and safe. A pipewell or tube-well consists of a 5cm diameter tube inserted into the ground and capped with a iron or steel hand pump. The majority of the wells were sunk by the United Nations Children’s Fund, UNICEF. Ironically these wells led to the largest arsenic contamination crisis in the world. In later years, privately sunk wells became more prominent, eventually outnumbering public wells. Currently more than 90% of the drinking water in Bangladesh derives from aquifers less than 300m deep, with most aquifers less than 100 meters deep.
In the 1980s health problems associated with arsenic poisoning were discovered in West Bengal. Despite these clues, the arsenic problem remained unknown until a 1993 examination of pipewell water n the Nawabganj district led to the discovery of high arsenic concentrations. The number of people drinking water from wells contaminated by arsenic is staggering. 27% of the shallow pipewells have concentrations of arsenic exceeding the Bangladeshi standards of 50µg/liter, which is five times the World Health Organization’s standard of 10µg/liter. It is estimated that up to 30-35 million people in Bangladesh and 6 million people in West Bengal are exposed to 50µg/liter arsenic in their water or more. 57 million people in Bangladesh are estimated to be exposed to 10µg/liter or more.
The crisis in Bangladesh and West Bengal highlights the health problems associated with arsenic poisoning. Skin problems such as keratosis, pigmentation and de-pigmentation, and skin cancer are widespread. Patients who have been exposed for a longer period of time have developed internal organ problems such as cancer, and many more have died. The arsenic poisoning was first identified in West Bengal in July of 1983. Since then, the numbers of arsenic victims has grown with each new study.
Nine districts in West Bengal, India, and 42 districts in Bangladesh have arsenic levels in groundwater above the World Health Organization maximum permissible limit of 50 µg/L. The area and population of the 42 districts in Bangladesh and the 9 districts in West Bengal are 92,106 km2 and 79.9 million and 38,865 km2 and 42.7 million, respectively.
A new study published Saturday in the British medical journal the Lancet found that tens of millions of people in Bangladesh have been exposed to poisonous levels of arsenic from contaminated groundwater. Bangladesh has struggled with arsenic in its water supply since a disastrous campaign in the 1970s to bring clean water to the county backfired horribly. Millions of tube wells were drilled to provide villagers with clean water, but many of them were dug into shallow layers of ground that had naturally occurring arsenic, contaminating the water. The Lancet study puts a figure on the toll from arsenic poisoning—and it’s astonishing. The study team, led by Dr. Habibul Ahsan of the University of Chicago, found that as many as 77 million people—half the population of crowded Bangladesh—may have been exposed to toxic levels of arsenic.
Ashan and his colleagues followed nearly 12,000 Bangladeshis over the court of 10 years and found that more than 20% of deaths were caused by arsenic:
They found that in the top 25 percent of people with the highest arsenic exposure, the risk of dying during the six years increased by nearly 70 percent compared with people with low arsenic levels.
People who drank moderate levels of arsenic were more likely to die from chronic disease than those who took in an amount within World Health Organization recommendations of 10 micrograms per literChronic arsenic exposure can lead to heart disease and cancers of the liver, kidney, bladders and skin—but the researchers found that arsenic could hasten death even at relatively low levels of exposure:
Compared to those exposed to the lowest arsenic levels (less than 10 microgrammes of arsenic per litre of water), those with levels of 10-50 microgrammes had a 34 percent higher risk of death, and those with the highest level (between 150 and 864 microgrammes) a 64-percent higher risk.
But even exposure at relatively lower levels carried a risk, a finding that is important for other countries — there are more than 70 of them around the world, including the United States, India and Mexico — that face a serious arsenic problem.What’s going on in Bangladesh is a unique horror—the World Health Organization has called it “the largest mass poisoning of a population in history“—and it’s partially due to the fact that Bangladesh gets 90% of its water from the ground. But what’s going on there is hardly unique. More than 70 countries around the world have issues with arsenic in their groundwater— and it’s not just poor countries like Bangladesh (Time, June 19, 2010).
What is Arsenic?
Arsenic – a metalloid element – is a natural part of the earth's crust in some parts of the world and may be found in water that has flowed through arsenic-rich rocks. Arsenic is also emitted into the atmosphere by high-temperature processes such as coal-fired power generation plants, burning vegetation and volcanic action. High concentrations of arsenic in drinking-water are found in various parts of the world including Argentina, Bangladesh, Chile, China, Hungary, India (West Bengal), Mexico, Nepal, Pakistan, Thailand, USA, and Viet Nam. A variety of instrumental techniques available for the determination of arsenic in water and air. (WHO Environmental Health Criteria, No. 224: Arsenic).
There is a theory that Napoleon Bonaparte suffered from arsenic poisoning, and samples of his hair did show high levels of the element. This, however, does not imply deliberate poisoning by Napoleon's enemies: Copper arsenate has been used as a pigment in some wallpapers, and microbiological liberation of the arsenic into the immediate environment would be possible. The case is equivocal, in the absence of clearly authenticated samples of the wallpaper.
Even without contaminated wallpaper, there are many other routes by which he could have picked up arsenic: arsenic was used medicinally for centuries and, in fact, was used extensively to treat syphilis before penicillin was introduced; it was replaced for treating other conditions by sulfa drugs and then by antibiotics. Arsenic was an ingredient in many tonics (or "patent medicines"), just as coca (unrefined cocaine) was an ingredient in Coca-Cola when it was introduced.
Carcinogen category notice: Category 1. Established human carcinogen known to be carcinogenic to humans. There is sufficient evidence to establish a causal association between human exposure to these substances and the development of cancer.
Carcinogen Category 1 (Confirmed Human Carcinogen)The heaviest occupational exposure to arsenic has traditionally been in copper smelters, but arsenic is also used in the microelectronicsindustry, in glass production, in pesticides, for wood impregnation and in tanning.
Because arsenic is a recognised carcinogen, the scientific and regulatory focus has been on cancer risks. Studies have also examined effects on atherosclerotic diseases and peripheral vascular diseases in different geographical areas and under varying exposure conditions. In this paper, we reconsider data from an epidemiological study that was conducted in Bangladesh (Rahman et al., 1999a,b; Tondel et al., 1999) and present some additional evaluations regarding exposure to arsenic through drinking water, skin lesions and the prevalence of hypertension and glucosuria.Degrees of toxicity:
As (III) > As (V) > Organic arsenic compounds.Arsenic poisoning does cause a variety of systemic problems when and if an individual does get the toxic of arsenic poisoning. The typical symptoms are; diaphoresis, muscle spasms, nausea, vomiting, abdominal pain, garlic odour to the breath, diarrhoea, anuria, dehydration, hypertension, cardiovascular collapse, aplastic anaemia and death. The degree to which symptoms a person has will be determined by the severity of the exposure.
Possible methods of exposure to toxic substances is common to all products. The possible methods of exposure are contact, ingestion and inhalation.
The first method is by contact and when the substances is arsenic the initial complication is a corrosive effect to the dermal layers. Over a prolonged contact exposure the resulting symptoms can be very dangerous and can cause focal hyperaemia, which means it decreases to blood flow to your arteries and veins and vesicular eruptions.





The second possible method of poisoning with an arsenic compound is by ingestion. The ingestion of arsenic will typically lead to the development of symptoms within thirty minutes. The initial symptoms may include a metallic taste in the mouth, hypersalivation, and dysphagia. The progression of symptoms would then include; vomiting, cramps, diaphoresis, breath odour (garlic like), and diarrhoea. If the exposure was of a large concentration then the progression of the arsenic poisoning event would lead to seizures, electrolyte disturbances and systemic shock. An exposure of an individual to arsenic that has resulted from a large quantity or concentration usually will result in death. If death does not occur with in a few hours then death will occur during the next few days due to renal failure.
The third method of exposure is by inhalation. The inhalation of arsenic compounds can lead to inflammation of the mucous membranes of the nasal and oral pharyngeal passage ways. The process may be delayed by this type of exposure because the concentration may be lower, but the end result will be the same symptoms as arsenic poisoning by contact, and by ingestion . Regardless of the method of the exposure toxic event can end in the same result, death!
Grade I Mild a) Diffuse melanosis. b) Suspicious spotty depigmentation / pigmentation over trunk/limbs c) Mild diffuse thickening of soles and palms. Grade II Moderate a)Definite spotty pigmentation /depigmentation on the trunk and limbs, bilaterally distributed. b) Severe diffuse thickening (with/without wart like nodules of the palms and soles). Gradelll Severe a) Definite spotty pigmentation/depigmentation as above with few blotchy pigmented/depigmented macular patches over trunks or limbs b) Pigmentation involving the undersurface of tongue and/or buccal mucosa. c) Larger nodules over thickened palms and soles occasionally over dorsal aspect of hands and feet. Diffuse verrucous lesions of the soles with cracks and fissures and keratotic horns over palms/soles.
Guha Mazumder et. al 2001Tani, 1999 classified affected villagers as 1 were suffering from malanosis (hypopigmentation and hyperpigmentation). Villagers in category 2 were suffering from melanosis and keratosis on the hands and/or feet. Villagers in category 3 were the most severely affected and were suffering from melanosis and developed (late stage) keratosis on the hands and/or feet. This classification is similar to that proposed by A.W Khan (WHO 1997). He suggested that arsenicosis could be categorised into 3 sequential stages:
1. Melanosis; 2. Keratosis with or without anaemia, conjunctivitis, bronchitis, gastroenteritis and blackfoot disease; 3. Developed keratosis and skin cancer. Arsenic is a metal compound that can easily find its way into the environment and the human population. The substance is found in our water, soil, food products. Even though we have governmental guidelines for controlling such toxic "substances" or "compounds" on a daily basis, we drink contaminated water and eat contaminated food products. This will lead to some degree of arsenic poisoning in each of us, according to Joe Harrison the technical director of Water Quality Association. Daily consumption of water with greater than 50 micrograms per liter of arsenic less than 1 % of the fatal dose, can lead to problems with skin, circulatory and nervous systems3. Greater problems can occur if the arsenic poisoning is of a chronic nature and resulting in neural disorders, vital organ damage and eventually death.
Arsenic is a compound that should be more closely monitored by parents, teachers and children because of its fatal results. The three main methods of exposure are contact, ingestion and inhalation. Regardless of the method of exposure all can produce basically the same symptoms.
WILL ARSENIC IN MY WATER CAUSE HEALTH PROBLEMS
If you are exposed to arsenic, several factors that work in combination with each other will determine whether harmful health effects may occur. These factors are:
- DOSE How much arsenic am I exposed to?
- DURATION How long and how often have I been exposed?
- TYPE of ARSENIC Have I been exposed to inorganic or organic arsenic?
GENERAL HEALTH, NUTRITIONAL STATUS, AGE, and LIFESTYLE
Some people may be affected by lower levels of arsenic than others. Young children, the elderly, people with long-term illnesses, and unborn babies are at greatest risk of being affected. They can be more sensitive to chemical exposures. Babies are not exposed to arsenic through breast milk at levels of concern even when their mothers have been exposed.
WHAT ARE THE HEALTH EFFECTS ASSOCIATED WITH ARSENIC EXPOSURE?


Based on studies in other countries, long-term exposure to high arsenic levels in drinking water has caused the following health effects:
- THICKENING and DISCOLORATION of the SKIN. Sometimes these changes can lead to skin cancers. These cancers can be easily cured if discovered early.
- STOMACH PAIN, NAUSEA, VOMITING and DIARRHOEA.
- NUMBNESS in the HANDS and FEET.
Many of the health effects of arsenic exposure are often seen with other common illnesses, which makes it difficult for a doctor to recognise. If you or your family members are concerned about health problems you believe are related to arsenic in your well water, you should discuss them with your doctor. You should also consider having your well water tested.
TOXICOKINETICSThe half-life of inorganic arsenic in blood is about 2 hours; the half-life of the methylated metabolites range from 5 to 20 hours.
Absorption
Pentavalent arsenic is well absorbed through the gut, but the trivalent form is more lipid soluble. Toxicity results from the arsenite form (As+3), especially by dermal absorption. Inhalation can result in symptomatic chronic exposure, particularly with arsine gas, which causes severe symptom by inhalation. Arsenic compounds are well absorbed parenterally within 24 hours.
The absorption of small doses of so-called toxins that would be without noticeable consequence if they are eliminated normally, wil, after a time, lead to a toxic threshold concentration being reached in the target organ or tissue, causing disorders in which the symtoms are highly variable.Distribution
Arsenic initially localizes in the blood bound to globulin. Redistribution occurs within 24 hours to the liver, lungs, intestinal wall, and spleen, where arsenic binds to the sulfhydryl groups of tissue proteins. Only small amounts of arsenic penetrate the blood-brain barrier. Arsenic replaces phosphorus in the bone where it may remain for years. Within 30 hours postingestion, arsenic deposits in the hair. Arsenic levels in hair sections may provide an indication of the time of exposure based on length from growth site. The hair of an individual who died 6 to 8 hours after ingestion of an arsenic overdose generally does not contain arsenic.
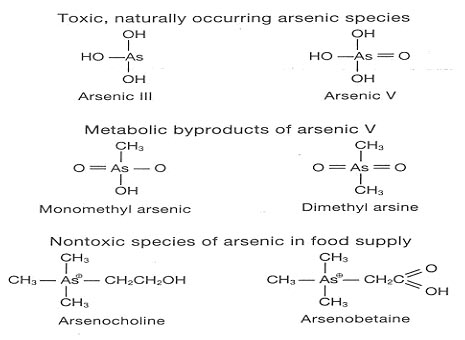
Organic Arsenic Sources
The two most commonly found organic, nontoxic variants of arsenic found in food regularly consumed by humans are arsenobetaine and arsenocholine. Considerable concentrations of organic acid are found in shellfish, cod, and haddock. After arsenobetaine and arsenocholine are ingested, they are rapidly cleared in the urine where they are completely excreted within 1 to 2 days (Fig. 1). No residual toxic metabolites are present. The half?life of organic arsenic is 4 to 6 hours.
Figure 1.
Pregnancy
Inorganic arsenic crosses the placenta. A 22 year old female at 20 weeks of gestation ingested 340 mg of sodium arsenate. The initial 24 hour urinary arsenic level was 3030 mg/L. Dimercaprol was administered. Fetal heart tones were normal. A healthy infant was delivered at 36 weeks. At birth 24 hour urinary arsenic levels were <50 mg/L in the infant and <100 mg/L in the mother. Another case of maternal arsenic ingestion at 30 week gestation resulted in infant death shortly after birth. Dimercaprol appears to be the agent of choice. D penicillamine has been associated with teratogenicity.
Gastrointestinal Tract
Dilation of splanchnic vessels causes submucosal vesicle formation. Rupture of these vesicles leads to rice?water stools and bleeding. Subsequently, a protein?losing enteropathy may develop.
Despite aggressive management of arsenic intoxication and a rapid decrease in blood and urine arsenic levels, neurologic defects may persist. It appears that distribution into neural tissue is rapid and may be irreversible even with chelation.
Muscle
Fatal rhabdomyolysis dysfunction has been reported after an acute arsenic overdose.
Metabolic/Hepatic
Negative nitrogen balance, hepatic fatty degeneration, central necrosis and cirrhosis, antagonism of thyroid hormone.
Skin Appendages
Alopecia (late), brittle fingernails, Mees's lines (horizontal white lines that appear after exposed nail bed area grows to exterior).
Blackfoot DiseaseBlackfoot disease is a unique peripheral artery disease in an endemic area of chronic arsenicism on the southwest coast of Taiwan. Humic acid in well water may be the main cause of the disease. Platelet activation and hypercoagulability may play a role in causing this disease.
LABORATORY Analytic Methods
The current standard for arsenic analysis is atomic absorption spectroscopy, which measures total arsenic, does not distinguish between pentavalent, trivalent, or organic arsine.
Blood Levels
The short half?life of arsenic in the blood means that blood arsenic levels are less useful than urine levels unless exposure occurred on the same day. Serum (or blood) arsenic levels are detectable only during the first 2 to 4 hours after ingestion, after which arsenic in any form is not readily detected in blood or serum.
Inorganic AS+3 and AS+5
AS+3 is more toxic than AS+5. AS+3 and AS+5 are detected in the body shortly after ingestion. Monomethylarsine and dimethylarsine predominate more than 24 hours after ingestion. Urinary AS+3 and AS+5 levels present about 10 hours and return to normal in 20 hours. Urinary monomethylarsine and dimethylarsine levels peak at 40 to 60 hours and return to baseline in 6 to 20 days after ingestion. The half?life of inorganic arsenic in blood is 2 hours and that of the methylated metabolites 5 to 20 hours. Serum (or blood) arsenic levels are only detectable during the first 2 to 4 hours after ingestion.
Organic As (Fig. 1)
Arsenobetaine and arsenocholine have a half-life of about 4 hours and are completely excreted in I to 2 days.
Urine: No exposure-less than 25 mg/daily.
Toxic levels 50 to 50,000 mg daily.
After seafood-50 to 2,000 mg daily.
Hair Levels
Hair analysis for arsenic is a semireliable method for confirming chronic toxicity. It does not discriminate between externally deposited arsenic and arsenic found within the hair shaft.
Fingernails
Fingernail arsenic may provide an estimate of the air arsenic exposure for a worker.
Associations Between Drinking Water and Urinary Arsenic Levels and Skin Lesions in Bangladesh
The present study examined the associations between drinking water and urinary arsenic levels and skin lesions among 167 residents of three contiguous villages in Bangladesh. Thirty-six (21.6%) had skin lesions (melanosis, hyperkeratosis, or both), of which 13 (36.1\%) occurred in subjects who were currently drinking water containing concentrations of arsenic less than 50 µ g/L.
The risk for skin lesions in relation to the exposure estimates based on urinary arsenic was elevated more than 3-fold, with the odds ratios for the highest versus the lowest quartiles being 3.6 (95% confidence interval, 1.2 to 12.1) for urinary total arsenic and 3.2 (95% confidence interval, 1.1 to 10.0) for urinary creatinine-adjusted total arsenic. The risks for skin lesions in relation to the exposure estimates based on arsenic in drinking water were less strongly elevated, with the odds ratios for the highest versus the lowest quartiles of exposure being 1.7 (95% confidence interval, 0.6 to 5.1) for drinking-water arsenic and 2.3 for cumulative arsenic index.
The study suggests that arsenic exposure is associated with skin lesions in the Bangladesh population and that urinary arsenic may be a stronger predictor of skin lesions than arsenic in drinking water in this population.(Habibul Ahsan, MD, Mmed Sc, Mary Perrin, MPH, Atiqur Rahman, MBBS, Faruque Parvez, MPH, Martin Stute, PhD, Yan Zheng, PhD, Abul Hasnat Milton, MBBS, MSc, Paul Brandt-Rauf, ScD, MD, DrPH, Alexander van Geen, PhD, and Joseph Graziano, PhD, Columbia University Medical Center, 2000).
). These skin lesions have also been considered to be an indicator of high exposure, and to constitute a pre-cancerous condition. Advanced keratosis is painful and results in disfigurement that can lead to social isolation. The high exposure to arsenic poses a public health problem in Bangladesh that has only recently attracted interest from the world. This situation seems to be one of the largest arsenic calamities of the world, with 30-70 million people in Bangladesh currently consuming arsenic-contaminated water (Chowdhury et al.,2000; Smith et al., 2000).
PROGRAM IN ARSENIC HEALTH EFFECTS RESEARCH
Researches at the University California, PROGRAM IN ARSENIC HEALTH EFFECTS RESEARCH School of Public Health and Centre for Occupational and Environmental Health University of California, Berkeley (1998) provided the following accomplishment on arsenic studies:
- Provided definitive evidence (from studies conducted in Argentina and Chile) that arsenic is a potent cause of human bladder cancer.
- Provided definitive evidence (from studies conducted in Argentina and Chile) that arsenic is a potent cause of human lung cancer.
- Demonstrated results which indicate that epidemiological and experimental human data do not support the methylation hypothesis.
- Showed that with exposure to water containing around 600 µµg/L, 1 in 10 adult cancer deaths may be due to arsenic-caused cancers, the highest environmental cancer risk ever reported.
- Identified a dose-response relationship between arsenic exposure and bladder cell micronuclei, a genotoxic marker of effect.
- Identified a preliminary dose-response relationship between arsenic concentration in well water in India and the occurrence of keratoses and hyperpigmentation.
- Studies currently underway in India, Chile and the US, will allow projection of cancer risks with individual exposure data.
NONMALIGNANT HEALTH EFFECTS OF ARSENIC EXPOSURE.
This thesis comprises a series of studies concerning occupational and environmental exposure to arsenic and some novel chronic health effects of this element, namely diabetes mellitus and hypertension. Substantial prevalence of the well-known skin manifestations of arsenic ingestion was also found to occur as a result of environmental exposure through drinking water.
Two case-control studies on diabetes mellitus and occupational exposure to arsenic included individuals employed at a copper smelting industry (Paper I) and in art glassworks (Paper II) in Sweden. Although the number of smelter workers involved was small (12 cases and 31 controls), a significant exposure-response trend was obtained (p = 0.03). The assessment of arsenic exposure among 888 glass workers was less detailed, nonetheless it revealed an approximately doubled risk (MH-OR = 2.1; 95% confidence interval 1.2-3.7) for the workers with occupational titles that suggested exposure. Overall, the results of these studies provide evidence that occupational arsenic exposure may play a role in the development of diabetes mellitus.
Four cross-sectional studies were carried out in Bangladesh, where a fairly large part of the population is exposed to inorganic arsenic in drinking water. In the first study (Paper III), the prevalence of diabetes mellitus among subjects with keratosis (n = 163) was compared with unexposed subjects (n = 854); keratosis was considered to be a definite sign of exposure.
A dose-response relationship was found between categories of time-weighted arsenic exposure (mg/L in drinking water) and the prevalence of diabetes mellitus (p < 0.001), and the crude overall prevalence ratio amounted to 4.4. Despite the lack of detailed individual exposure data and information on potential confounders other than age, sex, and body mass index (BMI), the association seems strong enough to support a causal relationship, because the adjusted overall prevalence ratio was 5.9 (95% confidence interval 2.9-11.6).
One of the other studies performed in Bangladesh (Paper V; 1481 exposed individuals, 430 exhibiting keratosis) showed a somewhat higher prevalence rate of skin lesions in males (31%) than females (26%) due to chronic arsenic toxicity.
The crude overall prevalence was 29% in the studied villages, and there was a distinct dose-response relationship between arsenic concentrations in drinking water and skin lesions (p < 0.01).
A clear dose-response relationship was also observed (Paper VI) between arsenic exposure and glucosuria for subjects both with and without skin lesions (p < 0.01). The possibility of using the skin lesions for initial screening for glucosuria was considered. However, the appearance of dermatological signs of chronic arsenic toxicity proved to be a poor marker in this respect, because glucosuria also occurred in the absence of skin lesions.
A third Bangladeshi study (Paper IV) indicated a significantly increased risk of hypertension in connection with exposure to inorganic arsenic in drinking water (1481 exposed and 114 unexposed subjects). The overall crude prevalence ratio of hypertension amounted to 1.7, and the adjusted (for age, sex, and BMI) ratio was 1.9 (95% confidence interval 1.0-3.6). A significant trend in risk (p << 0.001) was observed between an approximate time-weighted mean exposure to arsenic, considered in milligrams per liter or milligram-years per liter, which strengthens the possibility of a causal association.
(Mahfuzar Rahman , Akademisk Avhandling,Environ Health Perspect 1999 Sep;107(9):727-729 Department of Health and Environment, Faculty of Health Scien
ces, Linköping University)Why is Arsenic Bad for Health?
Arsenic dissolved in water is acutely toxic and can lead to a number of health problems. Long-term exposure to arsenic in drinking-water causes increased risks of cancer in the skin, lungs, bladder and kidney. It also leads to other skin-related problems such hyperkeratosis and changes in pigmentation. Consumption of arsenic also leads to disturbance of the cardiovascular and nervous system functions and eventually leads to death. These health effects – sometimes collectively referred to as arsenicosis – have been demonstrated in many studies. Increased risks of lung and bladder cancer and of arsenic-associated skin lesions have been reported for consuming drinking-water with arsenic concentrations equal to or greater than 50 parts per billion (or microgram per liter). (WHO Environmental Health Criteria, No. 224: Arsenic).
Arsenicosis is recognizable from skin colour changes, blotches all over the face and body, hyper pigmentation on the chest and upper arms, hard patches on palms and soles of the feet, inability to walk, debilitating pain, watery eyes
Arsenicosis, or arsenic toxicity, develops after two to five years of exposure to arsenic contaminated drinking water, depending on the amount of water consumption and arsenic concentration in water. Initially, the skin begins to darken (called diffuse melanosis). This happens first in the palms. Diffuse melanosis leads to spotted melanosis, when darkened spots begin to appear on the chest, back and limbs, although the latter is what is usual among people, and so is taken to be an early symptom. At a later stage, leucomelanosis sets in: the body begins to show black and white spots.
Keratosis is the middle stage of arsenicosis. The skin, in portions, becomes hard and fibrous; it is as if the body has broken out into hard boils, or ulcers. Diffuse or nodular keratosis on the palm of the hand or sole of the foot is a sign of moderately severe toxicity. Rough dry skin, often with palpable nodules on hands, feet and legs means severe toxicity. This can lead to the formation of gangrene, and cancer.
Arsenic poisoning brings with it other complications: liver and spleen enlargement and cirrhosis of the liver; myocardial degeneration and cardiac failure; peripheral neuropathy affecting primary sensory functions; diabetes mellitus and goitre; and skin cancers.
Three types of skin cancers are observed: Bowen’s disease (form of squamous cell carcinoma); basal cell carcinoma and squamous cell carcinoma. These cancers develop primarily from keratosis.
"Another unfortunate and complicating fact about arsenic poisoning," Hiroki Hashizume adds, "is that it generally takes from seven to 10 years, sometimes longer, for the disease to be recognized. When it finally is, it may be too late to treat." Professor Robert Goyer, who headed a nine-member commission of the US National Academies of Science, says its findings bolster a 1999 study by the Academy that found that men and women who drink every day water with 10 ppb of arsenic have an increased risk of more than 3 in 1000 of developing bladder or lung cancer during their lifetime. That risk rises to 7 in 1000 at 20 ppb.
WHO reports(Sept. 8, 2000):
Bangladesh is facing the largest mass poisoning of a population in history because of arsenic contamination of its drinking water supplies. The research by Allan H. Smith, professor of epidemiology at the University of California at Berkeley, said that between 33 and 77 millions of Bangladesh's 125 million population was at risk. Smith predicted a big increase over the coming years in the number of cases of disease caused by arsenic. These ranged from skin lesions to cancers of the bladder, kidney, lung and skin to cardiovascular problems. Bangladesh is grappling with the largest mass poisoning of a population in history because groundwater used for drinking has been contaminated with naturally occurring inorganic arsenic. The scale of this environmental disaster is greater than any seen before. It is beyond the accidents at Bhopal, India, in 1984 and Chernobyl, Ukraine, in 1986 (Smith).
The Bangladesh Observer adds (editorial, 17. 02. 03):
Though the mere mention of cancer brings the image of death, the fact is that in the case of children, around 70 per cent cases of cancer can be cured if treatment is provided at the right time. Ashic (A Shelter for Helpless Children) disclosed at a press conference that every year 2,50,000 children are affected by cancer and added that in 80 per cent of the cases, children are deprived of treatment as proper diagnosis is not done. We are also greatly alarmed to find that in the Bangladesh context between 5000 and 6000 children below the age of 15 become afflicted. A more searching look informs us that one child in 600 develops cancer before reaching the age of nine.
Mass majority of the rural population does not have any alternative. While those problems remain unsolved, thousands of villagers in Bangladesh will never be able to recover from a condition that has ruined their lives. "For the last ten years I've had spots on my body," says one villager, Aleya Begum, "but it's only recently that it has become a lot worse. Now, it feels that my body is burning and a continuous itching which I'm told won't go away for the rest of my life."
A neighbour, Iqbal Hossain, has a similar story. "In this village of ours, nearly three thousand people are living and about twenty-five people have been subjected to arsenic poisoning. Among them my condition is the most severe. Although the government had committed to supply arsenic free water two years ago, that commitment has not been fulfilled yet. The villagers didn't take notice of this problem at the beginning and now, although they are trying to stay free from arsenic poisoning, there is no way to resist it."
While the number of arsenic victims is increasing, so too is the level of acrimony as to who is responsible for this humanitarian disaster. The British Geological Survey is currently being sued by a Bangladeshi non-governmental organization. It allegedly conducted a survey in 1992 which revealed large quantities of arsenic, yet failed to provide thousands of villagers with adequate warning (Sakil Faizullah, 26 September 2002).
The regulatory regime in Bangladesh entangles in a number of governance issues... The rules as followed by the bureaucrats are, in most cases, outdated, complicated, ineffective and provide no scope for monitoring, transparency and above all accountability. (Patel, P. H., 2001).
You can’t go into a village and just screen. Say, as it has happened in many cases, that you have 100% of the tube wells contaminated. So one day people are very happily drinking from what they think to be safe sources and the next day an organization like BRAC or any other NGO, goes over and paints all the tube wells red because they’re contaminated far higher than the WHO or the Bangladesh standards. And they, the people, are left scratching their heads, "Where do we drink water from?" (B. Kabir, The world Bank, 2001)
Over 38,000 people affected with arsenic-related diseases
Arsenic Affects the Whole Body
KHULNA, June 24, 2008 (UNB): Over 38,000 people in the country were affected with arsenic-related diseases while water of 30 per cent tubewells contaminated with arsenic till 2006, according to a government survey. The number of patients may rise if the latest results of the division wise surveys are published, said a Health Department workshop here Tuesday.
Arsenic Programme of the Health Ministry and Department held the monitoring and evaluation workshop on "Searching of Arsenicosis Patients and Management". It also said Water of some 1.44 million tube-wells in 270 upazilas of 62 districts were contaminated with arsenic while 66.0 million tubewells identified as vulnerable.
Dr AKM Mujibur Rahman, NCD and OPHE Programme Officer, presided the workshop, addressed, among others, by Deputy Secretary (Administra-tion) of Health and Family Welfare Mahfuzul Huq, Divisional Deputy Director of Health Department Dr Zebunnesa Khatun and district Civil Surgeon Dr Maksuda Begum. In Bangladesh, arsenic contamination of ground water was first detected in 1993 by the Department of Public Health Engineering (DPHE) at Sama village of Baroghoria union in Sadar Upazila of Chapainawabganj district. After testing water in different districts, some eight arsenic patients were detected in 1995. The number rose to 23 in 1996 while 42 in '97 and 60 in 98. And the number stood at 38,412 in 2006. Some 5,120 arsenicosis patients were detected in Khulna division due to consumption of arsenic contaminated water. District-wise break up of patients are : Khulna - 420, Jessore - 1,537, Bagerhat - 490, Satkhira - 194, Narail - 107, Magura - 174, Jhenidah - 312, Chuadanga - 815, Kushtia - 637 and Meherpur - 373. The workshop was informed that the government has undertaken different arsenic mitigation programmes. Medicines have already been sent to different district and upazila health complexes through CMSD. The government has initiated to take rehabilitation programme for the arsenicosis patients. (The Financial Express, June 25, 2008).
Contaminated water has affected people in Bangladesh Arsenic poisoning through contaminated drinking water can lead to diseased arteries, which in turn can cause heart attacks and strokes, research shows.
Scientists say they have identified a link between long-term exposure to arsenic and the accelerated development of atherosclerosis or progressive narrowing and hardening of the arteries leading to the brain.
The findings, published in the Journal of the American Heart Association, strongly point to arsenic and possibly other pollutants, as risk factors for blood vessel disease throughout the body.
Lewis DR, Calderon RL. US Environmental Protection Agency, Human Studies Division, USA, 1999:
Human health effects potentially due to drinking water arsenic (As) are more frequently reported in other countries than in the United States (U.S.). The types of health effects reported in other countries, especially skin effects, are very different from outcomes observed in the U.S.
Results of a recent cohort mortality analysis among a historic population of 4,058 Latter Day Saints in Utah and historic As concentrations have found significantly increased mortality for all heart disease (Relative Risk (RR) = 1.26, 95% Confidence Interval (CI) = 1.03-1.55), respiratory cancer (RR=3.55, 95%CI = 1.37-9.20), and prostate cancer (RR=l.98, 95%CI = 1.04-3.77) among males. Females had moderately increased mortality from cerebrovascular disease (RR=l.42, 95%CI=0.94-2.15) and hypertension with heart disease (RR=l.99, 95%CI = 0.82-4.81). A dose-response analysis of median drinking water As concentration by town and residence years showed an increase for prostate cancer with increased concentration.
Similar results for these effects have been found in non-U.S, populations. Future directions for the examination of drinking water As and health effects in the U.S. include an assessment of data needs from areas representing different geology, metabolic studies, and epidemiologic studies of As exposure in populations in areas with moderate As. This is an abstract of a proposed presentation and does not necessarily reflect EPA policy.
Low-level exposure to arsenic in drinking water is widespread in the United States and elsewhere. In New Hampshire, for instance, where 40% of the population's water supply comes from private wells, as much as 8% of the state (one-fifth of all private well users) may be exposed to arsenic concentrations between the U.S. Environmental Protection Agency's proposed standard of 10 parts per billion and the current standard of 50 parts per billion. At industrial sites and toxic waste sites--including over 70% of all Superfund waste sites--arsenic is usually found in combination with many other toxic chemicals, and it can leach into groundwater and find its way into drinking water.
Statistics of Arsenic Calamity
Total Number of districts in Bangladesh 64 Total Area of Bangladesh 148,393 sq.km Total Population of Bangladesh 120 Million GDP per capita (1998) US$260 WHO arsenic drinking water standard 0,01ppm Maximum permissible limit of arsenic in drinking water of Bangladesh 0,005pm Number of districts surveyed for arsenic contamination 64 Number of districts having arsenic above maximum permissible limit 59 Area of affected 59 districts 126,134 sq.km Population at risk of the affected districts 75 Million Potentially exposed population 24 Million Number of patients suffering from arsenicosis 7000 Total number of tubewells in Bangladesh 4 Million Source: BBS, Dhaka Community Hospital, NIPSOM, DPHE.
Affected tube-wells, 1999 Assuming 0.250 mg/litre as the mean content of arsenic in groundwater, a person who consumes 1500 ml of this water each day for 10 years will consume about 6 gm of arsenic only from water. It is reported in the literature that 3 to 25 grams of arsenic when consumed over 1 to 22 years produces hepatic damage in the form of cirrhosis and non-cirrhotic hypertension (Morris, et al., 1974). Considering the poor health situation of the majority of the population in Bangladesh and double the amount of water consumption it is very likely dose-response effects will be more severe and devastating.
The development of atherosclerosis in the arteriesChih-Hao Wang of the National Taiwan University and colleagues studied 463 people living in an area of Taiwan with high rates of arseniasis, or chronic arsenic poisoning. Scientists have tracked the amount of arsenic in well water in the region for more than four decades
The team found that three indices of long-term exposure to arsenic correlated directly with the amount of atherosclerosis present in the carotid arteries. People with the highest arsenic exposure, they report, had three times the risk of atherosclerosis as seen in those who were not exposed to the element. "Our results indicate that long-term arsenic exposure may lead to the progression or acceleration of carotid artery disease and most likely generalized artery disease in humans," Wang notes. Because this study occurred in a region characterized by extremely high levels of arsenic in drinking water, the lowest level of contamination examined was 50 micrograms per liter (Journal of the American Heart Association, 26. 03. 02).
Arsenic Contamination in Rice(IRRI) growing Countries
Now around these paddy fields a disguised evil has crushed the nation, a catastrophe that is more severe than flood or tidal storm, Chernobyl, Bhopal or any kind of disaster that human being has ever faced to a such large extent. Slowly, but severely, painful deaths are occurring and most of the rural population of Bangladesh do not know why! A poison that you cannot see or even smell in the drinking water is hardly thinkable for such a simple-minded nation. The decision to change (so called "improvement") their life-style comes from the luxurious offices of the richest capitals of the world. A modern agrochemical /technological based agricultural system was imposed on them about three decades ago but they were never consulted nor asked for their advice.
Rice - IRRI High Yield Producing Countries in River Plain faceing Arsenic Contamination
Priya Harish Patel, Harvard University, USA,( 2001) describes, "Where are we going to land?" I thought, inwardly panicking as acres and acres of water drew ever nearer with each passing second. At that moment, I recalled that Bangladesh was in fact the most densely populated country in the world and that 35 million people in this watery wonderland were suffering from lack of safe drinking water.
I ignored these distracting thoughts as my plane safely landed on a magically appearing island of hard ground. A week later, I was rudely awakened to the reality of Bangladeshi life when I visited a rural village.
There, within the wetlands and rivers that are Bangladesh, millions of people had erected little huts held up by hardy strips of bamboo.
And there, I saw my first arsenicosis patient - his hands and chest were discolored and three fingers had been cut off due to gangrene, a symptom of advanced, chronic arsenic-poisoning. Here, within this green haven, millions of people were and are still living in a kind of hell - a hell they cannot see, taste, or feel but which invades their bodies through the water they drink and will eventually kill them."Before the beginning of the century there were 15 countries in the world that had arsenic contamination in water.Four countries,Bangladesh,West Bengal —India, China,and Taiwan, had populations that were suffering seriously.
In fact, in the time span of only two years (2000 –2002) six more nations have found significant ground- water arsenic contamination.These are Cambodia, Lao People Democratic Republic, Pakistan, Myanmar, Vietnam, and Nepal.The International Arsenic Conference at San Diego (July, 2002 ) brought out a new aspect of this debacle. For the first time the serious situation of Bihar (another state of India in Middle Ganga Plain), was confirmed. This new discovery reveals that a good portion of the Ganges Plain,with an area of about 530,831 sq.km.,may be contaminated with arsenic.This area has a population of about 450 million (including Bangladesh) (Chakroborti, 2003)Bangladesh among top rice-eaters Bangladesh among top rice-eaters
show data prepared by the Food and Agriculture Organization (FAO).
Brunei Darussalam tops the list with per-capita rice consumption of 245 kilograms a year, according to Faostat, a regular food supply data prepared by the FAO, reports BSS.
Vietnam is in second position with an annual rice consumption of 166 kilograms while Laos is one notch ahead of Bangladesh with 163 kilograms per person. Two South Asian nations -- Sri Lanka and Nepal -- are behind Bangladesh in per-capita rice consumption.
Higher rates of rice consumption are seen in much of South and Southeast Asia, West Africa, Madagascar, and Guyana. Some of these countries have consumption rates of over 100 kilograms per person a year. Asia, the world's most populous continent, has high rates of rice consumption. China and India alone account for more than 50 percent of the world's rice consumption but they are far behind other Asian countries in per-capita rice consumption, says a report of the International Rice Research Institute (IRRI).
The FAO statistics show that each person in Bangladesh consumes 160 kilograms of rice a year, which is more than three times higher than the average global consumption rate of 50 kilograms. Myanmar and Cambodia are behind Bangladesh with annual consumption of 157 and 152 kilograms. India, Pakistan and Bhutan are not on the top 20 list while Sri Lanka and Nepal hold the 11th and 16th positions.
Thailand, a major rice-producer, is in the 9th position with an annual per-capita consumption of 103 kilograms, while China stands 18th with 77 kilograms. South Korea is at the bottom of the top 20 list with each person taking 76 kilograms of rice a year. Although per-capita consumption has always been high in Asia, it has more than doubled in the rest of the world over the last 50 years, says IRRI (Daily Star, December 12, 2011).Sylheti rice to have far lower arsenic concentrations
Back to Content
A team of scientists led by Dr Parvez Haris from De Montfort University, Leicester, UK is carrying out research to remove arsenic from water and identify ways of reducing human exposure to arsenic through diet. Haris and his team have already demonstrated that exposure to the more toxic inorganic arsenic species is greater in people who eat more rice.
In this latest work, the De Montfort University team – along with Dr Michael Watts from the British Geological Survey, Keyworth, Nottingham, UK – has identified varieties that are low in arsenic but high in essential trace elements such as selenium and zinc. Earlier studies showed high concentrations of arsenic in Bangladeshi rice, but the rice samples were mainly from regions where the irrigation water contains higher levels of arsenic.
The team carried out a detailed study on rice from the greater Sylhet region in the north-east of Bangladesh, which generally has a lower groundwater arsenic concentration.
The results showed Sylheti rice to have a far lower arsenic concentration than similar types of rice from other regions of Bangladesh. Results also showed that the arsenic concentration in aromatic rice was 40 percent less than non-aromatic varieties and that it also contained higher concentrations of the essential elements selenium and zinc. “This is a very important finding since consumption of certain types of aromatic rice will not only reduce human exposure to arsenic, but will also increase their intake of zinc and selenium,” says Dr Haris. “This is very good news for millions of Bangladeshis who are exposed to high concentration of arsenic through drinking water and rice and are also deficient in zinc and selenium.”
For someone consuming 500 grams of non-aromatic or aromatic rice from Sylhet, the daily intake of arsenic from rice would be approximately 48 percent and 69 percent lower, respectively, compared with consuming non-aromatic rice from other parts of Bangladesh. “Our identification of rice with very low arsenic concentration and higher quantities of essential elements is good news for the Bangladeshis and other communities where rice is a staple food but it is important to encourage a more balanced diet that is less dependent on rice,” Haris explains.
Aromatic rice is generally cultivated during the wet (aman) season and therefore is less dependent on the use of groundwater for irrigation. It also requires less fertilizer and pesticides. Haris recommends that the authorities in Bangladesh encourage farmers to cultivate more aromatic rice. Although the yield of aromatic rice is lower, the farmers will not need to spend much money on applying chemicals that could pollute the environment and harm their own health. “Furthermore, energy costs (electricity or diesel) will be lower as there will be less need for them to pump groundwater for irrigation,” Haris says (Daily Sun, 17 February 2013).
96% of Well Water is Undrinkable: Arsenic Concentration Found as high as 1.088 ppm
Many of the arsenic affected areas are located in the arid region (with the annual rainfall of 200-300 mm) of the Hetao Plain between the Yellow River on the south and the Inshan Mountains on the north. The Gobi Desert lies on the west.The Hetao region had been known as fertile farmland attracting immigration. However, in recent years, there are desolate villages here and there since the residents left having given up their houses and fields due to the prevailing diseases such as cardiopathy, the disorder of circulatory organ, or cancer."The mortality rate is high here", or "Many people are suffering from cancer in this village". During the survey, two cases each of Bowen's disease and stomach cancer were confirmed by pathological diagnosis. In the arsenic affected Shengli village of the Haizhiyan district of Wuyuan county, 40 people passed away during the 11 years from 1986 to 1996 in the sixth, seventh and twelfth hamlets. (Villages consist of hamlets, each hamlet containing around 200-300 people). Among the 40 deaths, 15 were due to cancers. According to the various research reports compiled by the end of 1995, arsenic contamination in Inner Mongolia spreads in 655 villages of 11 counties and 1,774 patients were confirmed (Guo Xiao-juan, 2001).
Nepal is a landlocked country in southern Asia, between China and India, with a total land area of 140,800 square kilometres. Topographic variations are extreme and the terrain has a general southward slope. The topography ranges from rugged high Himalaya in the north, to the central hill region, to the lower-lying Siwalik Range (south-central) and down to the 'terai' or flat river plain in the south.
Elevations range from greater than 8000 m (Mount Everest range) on the north border with China to 70 m (Kanchan Kalan, terai region) in the south. Nepal has eight of the ten highest mountains in the world.Many of the documented problems are related to pollution of both surface waters and shallow groundwaters from domestic, agricultural and industrial wastes. Much of the Nepalese population uses surface water for potable supply which is most vulnerable to pollution. Hence only 34% of the population are thought to have access to safe drinking water (NepalNet, 2001).
Shallow groundwaters are also at risk from contamination: pathogenic bacteria, pesticides, nitrate and industrial effluents (urban and periurban areas) are likely to be the greatest problems encountered.
Shallow groundwaters in the Kathmandu Valley in particular are reported to have been contaminated with industrial and domestic pollutants in recent years (Jacobson, 1996).The nature of the industrial effluents present is not known in detail, but the greatest sources are likely to be from the textiles and carpet-manufacturing industries. These may introduce effluents with high salinity and containing organic chemicals and some trace metals (from dyes and finishing treatments).
The chemistry of shallow groundwaters in the terai region depends to a large extent on the lithology of the sediments: the shallow aquifers are vulnerable to pollution if surface sediments are sandy and permeable, but less so if a protective layer of low permeability (clay or silt) is present.As the shallow aquifer is reported to be largely unconfined, the vulnerability to surface pollution may be relatively high, at least in some areas.
However, in some parts of the shallow aquifer of the terai, anaerobic conditions are observed as some shallow groundwater has high concentrations of arsenic iron.
Arsenic in the terai groundwaters is a newly emerging problem and although no arsenic-related health effects have been recognised in the region, sufficient concern has been raised among the government and NGOs to launch an arsenic and health testing programme. Deep groundwaters present in the Kathmandu Valley and the terai are also largely anaerobic and hence vulnerable to increased concentrations of iron, manganese, ammonium and possibly arsenic. However, to date, no high-arsenic deep groundwaters have been documented in these areas. Springs from the karstic limestone aquifers at depth in the Kathmandu Valley are reported to be of calcium-bicarbonate type with good chemical quality, although the amount of data is limited.Arsenic
Of the aquifers present in Nepal, those potentially at greatest risk from contamination with arsenic are the recent sediments of the terai region. A number of surveys of groundwater quality have revealed the presence of arsenic in some samples at concentrations above desirable limits. The Department of Water Supply and Sewerage (DWSS) found 1% of water sources analysed had arsenic concentrations of greater than 50 µg/l (the Indian and Bangladesh standard for arsenic in drinking water).
Highest concentrations were found in groundwater from the active floodplain of the River Koshi. The Nepal Red Cross Society (NRCS), from testing in 17 of the 20 terai districts, found some 3% of groundwater sources sampled had concentrations above 50 µg/l, the highest observed concentration being 205 µg/l and the worst affected districts being Nawalparasi (Western Region), Rautahat and Bara (Central Region) and Bardia (Midwestern Region). NRCS (2001) has listed these districts, together with Parsa, Rupandehi, Kapilbastu and Banke as priority areas for testing, water-supply mitigation and health screening.
Finnida found 12% and Tandukar found 9% of samples analysed in their respective investigations had concentrations exceeding 50 µg/l.The highest arsenic concentrations observed by Tandukar (2001) were around 120 µg/l, most of the high-arsenic samples being from the River Bagmati area. The high concentrations appear to occur in anaerobic groundwaters and are often associated with high dissolved iron concentrations (Tandukar, 2001).
From the available data, it appears that the arsenic contamination occurs in the shallow aquifers of the terai (tubewells completed at <50 m depth). Deeper tubewells appear to have lower arsenic concentrations (<10 µg/l), although it is stressed that the volume of available data for the deeper aquifer is so far very limited.
housands of people in the Asian island nation of Sri Lanka have been struck by a mysterious and deadly form of kidney disease. A new study points to a likely cause - pesticides and fertilisers.
The new study blames farm chemicals, which are cheap in Sri Lanka, thanks to government subsidies, and often overused. Cadmium is found in some fertilisers. Arsenic is an active ingredient in some pesticides.
Companies that import and sell pesticides and herbicides contest the government's conclusion. They point out that the government and WHO have not yet released their full study.
"We believe the evidence is not scientific enough to say that the pesticide is the main reason for this chronic kidney disease," says Senarath Kiriwaththuduwage, research and development manager at Crop Life Sri Lanka, an industry trade association. "These findings are not published in reputed scientific journals."(BBC, 18 September 2012 Last updated at 05:40 GMT ) Aniruddha Padaniya President of the Government Medical Officers' Association The WHO says it will publish the study in the coming months, but are still finalising details.I am Dr.Channa Jayasumana from department of Pharmacology,Faculty of medicine,Rajarata University of Sri Lanka. Here in Sri Lanka we are facing to such a similar problem as you are facing in Bangladesh. We found chronic arsenic poisoning among paddy farmers in Sri Lanka. We are having enough evidence to say source of arsenic is agrochemicals.We have already published several papers(Please find attached documents). I would like to build up a productive link with genuine Bangladesh scientists. Further I would like to draw your kind attention to our preliminary work
The prelimlnary lnvestigation, and clinical surveys conducted by the medical experts of the Minis{ry of Health appointed by DGHS reveled that there is prime-fascia evidence of chronic Arsenic Toxicity in some of the geographicar areas where there are diagnosed patients of cKDu are inhabitant. Further investigations into this matter which is seriously affecting the health of the people. The possible sources are fertilizer and pesticides used in agricurture industry.
Pesticides even containing minute quantities of Arsenic and Mercury are very Iikely to cause serious health effects due to environment contamination not only to users but also to the othei inhabitants of the locarity due to oro,oru;;;ro"r*" *, contamination with water. As far as we are aware, there is no safe rever for Arsenic as it is a Carcinogen. In recent years a significant increase in number of patients of Chronic Kidney Disease of unknown etiology (CKDu) has been observed in some parts of Sri Lanka, especially in the North Central Province.
A case control study has been performed with the intention of determining the prevalence of clinical features of Chronic Arsenic Toxicity (CAT) among CKDu patients in Padavi Sripura divisional secretarial area in Trincomalee District, Sri Lanka.
Clinical assessment were done in diagnosed CKDu patients (n=125) and non-CKDu persons (n=180) as the control group.
Hair and urine samples collected from both CKDu patients and controls were analyzed for presence of arsenic using Atomic Absorption Spectrometry equipped with Hydride generator (HG-AAS).
The results revealed that 68% of CKDu patients and 28% of the controls had urine arsenic levels above 21 ìg/g creatinine, which is considered the point of threshold for manifestation of early renal changes that can be developed in to chronic kidney disease.
Among the CKDu patients, 48% and 17.4% of the subjects in the control group have fulfilled the criteria to be diagnosed CAT, indicating the potential link between CAT and CKDu. Agrochemicals could be the possible source for this contamination of arsenic since no reported work is available to indicate the presence of arsenic in the bedrocks of Sri Lanka (Ministry of Health Sri Lanka,
June 08,2013, Colombo, Sri Lanka Guardian:
It is now established that Arsenic is present in at least some of the agrochemicals imported to Sri Lanka. Several tests by the research group at the University of Kelaniya headed by me, studying various aspects of the Rajarata Chronic Kidney Disease Unidentified Etiology (RCKD un et) has come across this finding, and at least one other group has confirmed these results. As the name indicates the cause of this disease is not identified in western medicine though many patients have deceased during the last few years. The research team at the University of Kelaniya, other than me consists of western Chemists, Botanists, Mathematicians who are employed as Professors and Senior Lecturers at the University of Kelaniya as well as those who practice western Medicine, some of whom are academics at the Rajarata University. We have made use of standard techniques in Atomic Absorption Spectrometry in almost all of the tests we have carried out at Kelaniya. Our research team had to explain (i) the spread of RCKD un et only in Rajarata area and (ii) the incidence of the disease only during the last twenty years. Various groups working on the RCKD have come up with causes such as Cadmium, Aluminum in the cooking utensils. However due to reasons not described here for want of space, our group has rejected all these "explanations" and we have all the reasons to come to the conclusion that Arsenic is the cause of the disease. Now the question may be asked as to how the Kelaniya group was able to detect Arsenic in Rajarata drinking water in the affected areas and in agrochemicals when the other groups were not able to do so. In fact we are also surprised that Arsenic had not been identified in agrochemicals, as only standard methods known to the western Chemists were used by us in detecting Arsenic in these products. It has to be mentioned that detection of Arsenic in drinking water in Rajarata that is contaminated with certain salts needs a special technique that has been developed at Kelaniya. We are more than surprised how these agrichemicals have been allowed to be imported and distributed in Sri Lanka when the authorities could have easily tested for Arsenic before the relevant products were released to the importers.
We have to distinguish between two cases here, they being the presence of Arsenic in drinking water in the relevant areas and the presence of the same in agrochemicals. As mentioned above the authorities should have tested for Arsenic in agrochemicals before they were allowed to be imported and distributed. Apparently the importers of the agrochemicals with Arsenic have declared to the Sri Lanka customs that Arsenic is not present probably based on information supplied to them by the exporters. Even if the exporters had claimed that there was no Arsenic present in the relevant agrochemicals, we are of the opinion that the importers and the authorities in Sri Lanka responsible for giving clearance should have tested independently for Arsenic knowing its deadly effects.
Our group at Kelaniya consists also of people who are interested in developing our own systems of knowledge and in this respect we not only create (or discover as many are accustomed to that term) our own theories (ape pravada), rather than being satisfied with being mere tinkerers of western knowledge in the periphery, and we have been successful at least in a few instances. During the last two years or so we have come across another source of knowledge, namely the "samyak drushtika devivaru" who communicate knowledge when necessary to a lady who is known to us. Those who have been brought up in the western scientific tradition would laugh at this source of knowledge, but we are in a position to debate with them on this matter publicly not in a five star hotel, but in a place such as the Public Library Auditorium, if they are not happy with the "samyak drushtika devivaru". The communicator does not go into a trance or any such peculiar position (arudha, avesha etc.,) but communicates with the devivaru while she is in conversation with the others.
I had been thinking of Bhavana as a means of acquiring knowledge for some time but did not know how or where to begin. Under the instructions of the devivaru (I do not want to use the word gods as the word has many connotations) few among us (I do not have that "vasana" probably due to my karma) are able to "experience" knowledge after engaging in Bhavana, and the devivaru and these people with "vasana" (it is not luck for anybody’s sake) have diagnosed deceases and treated successfully patients who had been turned away by the western medical personnel. I do not want to go into details at present but we will present our story to the public in due course. What is emphasized here is that neither nobodies nor some bodies could acquire this knowledge through Bhavana as only those who are "endowed" with the necessary "adhyathmica shakthiya" could do so.
It was the ‘devivaru’ who suggested to us that we should test for Arsenic in the water, soil, and even flora in the affected areas in Rajarata. Our group that consists of western trained scientists set about in the usual way as they have been instructed, to collect samples of water soil, plants etc., and tested for Arsenic in the laboratories in the Faculty of Science of the University of Kelaniya. We did not want to carry out these experiments without informing the rest of the academics in the Faculty of Science, and as the Dean of the Faculty I made it a point to make them aware of what our group has been doing. There was no opposition as such from these western trained ladies and gentlemen at the meetings of the Faculty Board though many "kathas" spread and a few people with vested interests tried to obstruct our work. They had even complained to the Minister of Higher Education and the President that a "devale" has been created in the Faculty of Science as we had commenced Bhavana sessions for students as well as staff (both academic and non academic). I suppose they wanted the Minister and the President to interfere with our work but the latter had decided to ignore these complains. I must say subsequently some members of the group met the President and that he is more than interested in our work.
It is true that the idea that Arsenic is present was given to us by the ‘devivaru’ but we do not want anybody else, especially those who are trained in the western scientific tradition to believe us or the devivaru. I must also add that there are some among us who could "see" Arsenic in the samples we collected from Rajarata area, with "adhyathmika shakthiya". However, we went through the standard methods in western Chemistry using the Atomic Absorption Spectrometer available at the University of Kelaniya to convince the western scientists of the presence of Arsenic. Unfortunately, the standard methods available in the text books and the journals did not help us to identify Arsenic in hard water in Rajarata areas, and then again the devivaru came to our rescue and suggested a particular method that could be adopted. Using this particular method, and using chemicals only, our group has been able to detect Arsenic (Arsenates) in the samples of hard water. I am only giving an outline of what our group has been doing and the details have been presented at seminars held at Rajarata University and the ministry of Technology and Research. I must also add not being a western scientist or a western academic in general my interest in the whole exercise is confined to epistemology as developed in our culture, in addition to finding a cure for the disease.
The western medical personnel in our group observed symptoms of Arsenic poisoning in the samples of patients whose number is around twenty thousand in Rajarata, especially in Mahavillacciya, Padavi Sri Pura, Padaviya, Vahalkada and surrounding areas. This led to tests in biological parts such as hair, fingernails from patients and kidneys removed from at least two people who died from RCKD un et. We have no reason to believe that Arsenic is not the cause of RCKD and we may now drop the tag un et that follows the name of the decease.
It was also found that the arsenate compounds responsible for the RCKD are formed only when Arsenic is mixed with hard water found in the Rajarata areas. This is the reason why the decease is confined to the Rajarata areas. As Arsenic is not found naturally in Sri Lankan soil, we wanted to find out how Arsenic got into the soil and the water in Rajarata. The suspect was nearer at hand and it was nothing other than the agrochemicals. We tested for Arsenic in agrochemicals using standard western Chemistry and the tests carried out have confirmed that Arsenic is present in these substances in high proportion. This explains why the RCKD is confined to the last twenty years or so as the effect of the agrochemicals which were first introduced in the sixties is felt during that period.
The Sri Lanka customs got interested in our work and they wanted us to test some samples of agrochemicals that they had acquired. Our group detected Arsenic in those samples as well, using again the standard methods in western Chemistry. When the importers had complained to the custom officers that the former would not believe in our results we took the unprecedented step of carrying out the chemical tests in the presence of a delegation of importers as we realized the gravity of the problem.
I would not say that our job is now over, as we have to work hard to get the authorities to cancel the license to import these agrochemicals contaminated with deadly Arsenic and also to cure the unfortunate citizens of our country who have been victims of "thanhadika" western manufacturers and local importers. There is a cure for the disease communicated to us by the devivaru, but unfortunately we do not have sufficient number of "vedanan" to attend to the victimized patients.
The largest mass poisoning, Bngladesh/India
The largest mass poisoning of a population in history is now underway in Bangladesh. It is a terrible public catastrophe, asserts Allan H. Smith, Professor of Epidemiology at the University of California, Berkeley, and a WHO consultant who has investigated arsenicosis in Bangladesh on several trips. The number of people affected by this arsenic disaster is among the greatest of any disease facing the world today. "By virtue of its sheer size it is pushing the limits of our knowledge and capacity to respond to it," asserts Professor Hans van Ginkel, Rector of the United Nations University in Tokyo (WHO,Friday 22 March 2002)
Why do people die in arsenic poisoning?
The contamination of wells with arsenic is one of the greatest environmental disasters being faced today and must rank as one of the worst in recent times. At the request of contacts in West Bengal I researched the matter and found a technology that can get rid of all traces of arsenic. Since then I have tried to mobilise public opinion to find finance for implementation and have also talked to the West Bengal Government, people and authorities in Bangladesh, US AID, UNICEF, DIFID, SIDA and other aid donors
My own estimate is that one person is dying every 15 minutes and millions are suffering in illness. But very few politicians and bureaucrats live in the affected villages and the people dying are considered to be of no consequence.
Worse still, the token efforts of the World Bank and other aid agencies has added obstacles to solving the problem. If the captain of the Titanic broadcast a May Day message, most of these people would have commissioned studies on iceberg flows and common sense home spun ways of avoiding icebergs rather than sending ships to take the passengers off.
My conclusion is that:(V. Chand, UK, 2003).
- the problem is chronic,
- the contamination is irreversible and worsening,
- no other safe water sources can substitute the wells,
- aid agencies helped produce the problem due to lack of care about environmental impact, and are today full of ill considered patronising solutions,
- the solution must fit village culture, be robust and be commercially sustainable,
- technology exists to solve the problem but it will cost a lot,
- no one cares sufficiently since its is all theoretical for them.
No body is willing to marry Rahima Khatun
The reason: She is a patient of arsenic-contamination. Over the past ten years, she has lost her parents and other family members owing to the same disease. Presently, she has one widowed sister, Mina Bewa, and her (Mina’s) two little sons. Rahima has contacted various diseases following the effect of arsenic. She lives at Sheikhpura village in Manikchak block and earns her livelihood working in fields. At times she has to beg to fetch food for her family members. Villagers know Rahima is on the verge of death. Because like Rahima, more than 10 villagers have died owing to arsenicosis and she is waiting for the same fate. Her next-door neighbour, 68-year-old Abdul Hanif, is suffering from arsenic-contaminated diseases.
But the plight of these villagers is that they do not get the scope to collect arsenic-free water from a distance point owing to irregular supply due to various technical reasons. Unfortunately, despite poverty they have one tube well at their house and still they are drinking under ground water.Though a section is aware of the name of PHE water after setting up of an arsenic-free water treatment plant spending Rs 50 crore at Mathurapur in Manikchak block, very close to the village, but there was no sign of campaigning by any NGO group to stop using ground water. Having no alternative, villagers are drinking “a drop of poison”, as it were, every day.
But in the next village, another victim, middle-aged Soyeb Ali, who has lost his right hand, collects PHE water for drinking every day, according to the guidance of the state’s school of tropical medicine. Ali had to agree with Kolkata doctors to amputate his right hand and is tying hard to live a new life. Tafajul Hossain (40), a jobless man owing to arsenic-contamination, despite amputation of his right leg fingers is living an uncertain life with four children and wife at Sardaha village near Golapganj in Kaliachak III.At Bamongram village in Kaliachak I, where an NGO Chetana is working with the ‘Keratosis’ patients with vigorous toxicity, tested over 2,000 samples. The local youths are organising this clinic here every Wednesday and a group of homoeopathy doctors is doing its best applying medicines and advising safe drinking water to the patients. Dr Subrata Pal Choudhury and Dr Bidhan Mandal, doctors of the Chetana clinic, said: We are trying to find out how three-year-old babies are being affected by arsenic contamination. From this clinic we have several such babies who are affected by arsenic and its deposition is found in their hair and nail. Some babies are coming with genetic weakness with the effect of arsenic-contamination.”
On the other hand, people of arsenic-affected areas are suffering from diseases like gallbladder, bronchial, diabetics and other problems. As a result, the former sabhapati of Kaliachak I panchayat samiti, Noor Mohd. Biswas, died following attack of arsenic few years ago, a local practitioner, Dr Samuel said. A section of people in mostly affected zones is conscious about using under ground water in Kaliachak III and I. Some NGOs are also spreading awareness (The Statesman, Calcuuta, 2005).
Bihar wakes up to arsenic menace
PATNA: In the past couple of years, Ojhapatti village in Bhojpur district has seen only a few "baraats" or marriage processions. Nobody wants to marry a woman born and brought up in this village. And families with grown-up daughters are increasingly moving out of the village to get them married. In Bihar's heartland, Ojhapatti is one of the most affected villages by arsenic. The ground water in this sleepy, impoverished village is said to contain very high amounts of arsenic, about 50 parts per billion (PPB) which is five times more than the permissible 10 PPB (according to WHO and Bureau of Indian Standards).
Since the word has spread, men now hesitate marrying women brought up in this village for fear of having abnormal children. Even though the village has now a piped water supply system, which is rare in rural Bihar, the ostracism remains. Arsenic affects 11 of Bihar's 38 districts. It was first detected in Bhojpur district about four years ago after people began to pour into hospitals with symptoms of arsenic poisoning.
They all had dark pigmentation on their body with lesions on the soles and palms. Some were also detected with skin cancer. Sources said the state government has estimated an expenditure of Rs 324 crore over the next decade to provide a permanent alternative water supply network in the affected areas. Arsenic is erratically present in ground water. One tubewell may draw up highly contaminated water and another, barely 10 metre away, may be totally free of arsenic. After a recent survey, 11 districts starting from Bhagalpur in the east of the state to Bhojpur in the extreme west, all along the Gangetic plains, were declared arsenic-affected by the state government (Times of India, 24 June, 2006).
CSE finds arsenic contamination in Gangetic region
NEW DELHI, OCT. 5, 2004: The Centre for Science and Environment (CSE) today claimed that it had detected high levels of arsenic in the ground water westward along the Gangetic plains, with the Ballia district in Uttar Pradesh being particularly affected. While the Ballia administration denied this and even sent a legal notice to the CSE saying it was working against "national interest," the CSE director, Sunita Narain, said she stood by the findings and wants immediate remedial action by the State Government, including better monitoring of ground water.
The laboratory analysis of hand-pump water and the hair and nails of people living in the villages of Ballia has shown levels of arsenic much higher than what is considered safe, Ms. Narain said. Though there is no legal safe limit for arsenic in hair, toxicologists say between 80 to 250 parts per billion (ppb) is acceptable. The level of arsenic detected in human hair here was 4,800 ppb to 6,300 ppb.
The content of arsenic in ground water ranged between 15 ppb and 73 ppb, while the guidelines describe 10 ppb safe. Similarly, the acceptable level of arsenic in nails is between 430 ppb and 1,080 ppb but tests showed it was close to 2,480 ppb. The tests were conducted at the Delhi-based Shriram Institute of Industrial Research Laboratory. Ms. Narain presented a UNICEF survey and studies conducted at Jadavpur University, which showed that, besides West Bengal, arsenic was found in Bihar, Uttar Pradesh, Assam, Jharkhand and Chhattisgarh. According to the two studies, scientists believe that arsenic is present naturally and brought down from the Himalayas.
The CSE stumbled upon the possibility of the presence of arsenic in water when Dinanath, a resident of Ekwana Rajpur village in Ballia, came to the All India Institute of Medical Sciences (AIIMS) for cancer-detection tests. His sons and many other villagers were suffering from skin diseases related to arsenic poisoning. When the CSE team checked his hand-pump, the arsenic level was found to be 73 ppb as against 10 ppb set by the Bureau of Indian Standards.
As of now, the Central Government says that arsenic contamination is found only in eight districts of West Bengal and Bihar (Bhojpur). "The CSE believes that the case of Ballia highlights a matter of intense urgency to understand the extent of arsenic contamination in the country; and on this basis create a clear policy and action plan to ensure that people are not forced to drink arsenic contaminated water," Ms. Narain said ( Aarti Dhar, The Hindu, India, 2004).Arsenic affecting Bangladesh crops
Crops in Bangladesh are being contaminated with arsenic from water used for irrigation, according to research by Bangladeshi and Australian scientists. They found evidence of high concentrations of the poisonous substance in rice and vegetable plants. Contamination of drinking water affects around 20 million people in Bangladesh and the neighbouring Indian state of West Bengal.
Arsenic in Bangladesh drinking wells may be linked to crop irrigation,
MIT study finds ruthless killer in Bangladesh's drinking water is making millions of people sick and may be causing as many as 3,000 deaths each year. That killer--naturally occurring arsenic in the water drawn from family wells--appears to have been released through a process involving crop irrigation, at least in one part of the country. At a research site in the southern part of Bangladesh, scientists calculated that irrigation pumping, which began in the last several decades, has dramatically altered groundwater flow through the aquifer. They show that the resulting changes to the chemistry of the groundwater have the potential to either increase or decrease arsenic levels, in a paper written by an MIT-led team of scientists in the Nov. 22 issue of Science. "Our data indicate that the arsenic was mobilized largely by degradation of dissolved organic carbon by microbes. Some of the organic carbon appears to have been drawn into the aquifer by irrigation pumping," said Charles F. Harvey, assistant professor of civil and environmental engineering at MIT and lead author of that paper. "But the effects of irrigation are complex, probably lowering arsenic concentrations in other areas. Curtailing irrigation pumping is not a solution."
Harvey is also an author of a research paper providing an epidemiological analysis of arsenic-induced illness throughout Bangladesh. That paper will appear next year in the Water Resources Research journal published by the American Geophysical Union. In it, the authors conclude that replacing 31 percent of the country's most tainted wells with deeper wells will eliminate about 70 percent of the illness, assuming that arsenic levels remain low in the deep wells.
Arsenic poisoning, usually characterized by sores on the chest, or blackened knotty palms, and cases of skin, lung, liver, bladder and pancreas cancers have been linked to arsenic in the drinking water. In 1998 the World Bank agreed to provide Bangladesh a $32.4 million credit to develop a method of controlling the arsenic. But today, most Bangladeshis continue to drink arsenic-laced water. The World Bank describes the problem as one of the world's primary environmental challenges. The World Health Organization refers to it as "the largest mass poisoning of a population in history" in a fact sheet published in March.
The mass poisoning began, sadly enough, with a well-meaning attempt to provide clean drinking water for Bangladeshis, who suffered from cholera and other diseases caused by bacteria in water taken from surface reservoirs. To remedy that problem, the Bangladesh government, with the help of international aid organizations, drilled between 6 and 10 million wells at depths ranging from 50 to 300 feet to provide clean, safe water for individual households. At about the same time, farmers in this largely rural country began irrigating land so that rice, the country's main food staple, could be grown during all six of the dry months when monsoon flooding abates. Cholera deaths dropped. But about 10 years into the use of the tube wells, villagers started displaying symptoms consistent with arsenic-related illnesses, and incidents of skin cancer and internal cancers became common.Arsenic in paddy
ON January 14, 2010, The Daily Star reported an increase in the accumulation of arsenic levels in the topsoil of agricultural lands that are irrigated by arsenic-rich groundwater. The article referred to a recent study by Professor Badruzzaman and Professor Ali (both of Buet). In their study, the professors reported that paddy grown on lands that have been irrigated by arsenic-rich groundwater contain up to 0.3 milligrams (300 micrograms) of arsenic per kilogram of paddy. A relevant but unanswered question is whether this level of arsenic in the grains is a health threat. While the Daily Star article is rather ominous in its tone, some analysis based on WHO and FAO data leads to a less threatening conclusion.
World Health Organization (WHO) and Food and Agricultural Organization (FAO) have been concerned with arsenic for several decades now. In 1967, Who established the maximum allowable daily load (MADL) of arsenic as 50 micrograms/kg of bodyweight/day. Several years later, these initial limits were significantly revised by the Joint FAO/WHO Expert Committee on Food Additives (JECFA). The revision declared provisional tolerable weekly intake (PTWI) of 15 micrograms/kg of bodyweight/week for inorganic arsenic (the harmful form of arsenic generally found in the ground). Note that this translates to arsenic intake of just 2.14 micrograms/kg of bodyweight/day. This stringent limit set forth by JECFA remains in practice even now. It should also be noted here that the minimum lethal dose of arsenic is roughly 1,000 micrograms/kg of bodyweight/day.
With the different arsenic intake limits available, we are in a position to examine whether arsenic consumption through rice is a serious threat. Let us assume that the average Bangladeshi man weighs about 60 kg and the average woman weighs about 50 kg. Then, following the most stringent arsenic intake limit set by JECFA, we have PTWI of approximately 900 micrograms (128.57 micrograms per day) and 750 micrograms (107.14 micrograms per day) of arsenic for a man and a woman respectively. If we adhere to the 1967 MADL limit, MADL is 3,000 micrograms for a man and 2,500 micrograms for a woman. The minimum lethal dose would be about 60,000 micrograms for a man and 50,000 micrograms for a woman.
It is estimated that for average Bangladeshis, about 70% of daily caloric intake comes from rice. Assuming that a woman of 50 kg weight consumes 1,500 calories and a man of 60 kg weight consumes 2,000 calories, the woman will have consumed 1,050 calories in rice and the man will have consumed 1,400 calories in rice. Since 1 gram of rice produces 4 calories, we can deduce that the woman will have consumed 262.5 grams of rice and the man will have consumed 350 grams of rice per day.
If the rice comes from paddy that has 300 micrograms of arsenic (the highest amount found by Professors Badruzzaman and Ali), then the arsenic consumption for our hypothetical 60kg Bangladeshi man is 105 micrograms and for our hypothetical 50kg Bangladeshi woman is 78.5 micrograms per day. These numbers are below even the most stringent arsenic intake limits established by JECFA. Of course, the MADL and the lethal levels are nowhere near the arsenic consumed through rice that came from paddy registering the highest levels of arsenic in the study.
Although these levels of arsenic are below the PTWI established by JECFA, the health risks involved with considerable consumption of arsenic should not be neglected. As identified by the WHO, the symptoms associated with arsenic poisoning are abdominal pain, vomiting, and bloody "rice water" diarrhea. Also, arsenic is classified as a carcinogen and may cause cancer of the skin, lungs, kidneys, and bladder. The health risks of arsenic are greatest for children, elderly, and those whose immune systems are compromised due to disease.
In Bangladesh, arsenic intake occurs mainly through drinking arsenic-rich water. Reducing arsenic content in drinking water is an effective way to keep arsenic intake in check. Compared to the threat of arsenic-rich drinking water, the presence of arsenic in irrigation water (because it passes on to food grains) seems less threatening. Being aware of arsenic concentration in water is necessary, but a trace amount of arsenic in paddy is perhaps not as alarming.UNDERGROUND ACTIVITY
It is widely believed that the arsenic was transported on sediment into the Ganges delta from the Himalayan mountains, which border Bangladesh on the north. What scientists don't know is how the arsenic is released into water in the aquifers in such great quantities. WHO's guideline for a maximum amount of arsenic in drinking water is 10 parts per billion (ppb). Many of the wells in Bangladesh measure more than 50 ppb, though arsenic levels vary from well to well. If the arsenic is in the aquifer only at certain levels, then digging even deeper wells might solve the problem. The Harvey research team selected a site 30 km south of the nation's capital city, Dhaka, and 7 km north of the Ganges River. They installed 17 research wells about 4 meters apart at depths ranging from 5 to 165 meters, and collected three sediment cores, determining that the sediment was typical of southern Bangladesh.
They did not find peat, which has been associated with dissolved arsenic, but did find a fairly even distribution of solid arsenic in a variety of forms. To determine whether it was this arsenic that was mobilized in the aquifer, and figure out how that might have happened, the scientists injected test substances into their sampling wells, then took water samples to see how the water was affected. One such test substance injected through the tube wells into the aquifer is molasses, which is rich in organic carbon. In water samples taken over several months, they found that arsenic levels quickly rose, as the organic carbon or its degradation products mobilized arsenic from the sediment. Injections of nitrate and oxygen-rich water provided further data, showing that arsenic levels can drop quickly after introduction of an oxidant.
What remained was to find the source of the carbon. Harvey's team used radiocarbon dating to determine the age of the carbon isotopes in the groundwater at various depths. They found that very young and very old carbon were mixed, and concluded that water had carried young organic carbon (probably derived from untreated waste on the surface) deep into the aquifer.The second research project was the first detailed statistical analysis of the epidemiology of the health effects of arsenic in Bangladesh's groundwater. Using geostatistical methods, the scientists constructed a map of arsenic concentrations that divides Bangladesh into regions and estimates trends in arsenic concentration at various depths. Using census data to estimate exposure distributions in the regions, and epidemiological data from West Bengal and Taiwan--countries where the effects of arsenic poisoning from drinking water have been well-documented--they estimated what dose of arsenic makes people sick. The scientists predict that long-term exposure to present arsenic concentrations will result in approximately 1.2 million cases of hyperpigmentation, 600,000 cases of keratosis, 125,000 cases of skin cancer and 3,000 fatalities per year from internal cancers.
"These numbers are highly uncertain," said Harvey. "We put together available databases to see what they imply, but the dose-response models for Bangladesh remain very rough." The authors conclude that by replacing a selected 31 percent of the country's most-affected wells with deeper wells, arsenic poisoning and arsenic-induced cancers would be reduced by about 70 percent, assuming that arsenic concentrations in deep wells remain low. "If the arsenic levels remain low at greater depths, and I think they will, then deeper wells are a good solution. But this should be studied," said Harvey, who added that the best immediate solution is to filter the water.
Solving the arsenic problem in Bangladesh could also help people in other countries, such as those along the Mekong River delta in Vietnam, Laos and Cambodia, where high arsenic levels in drinking water and crop irrigation are becoming common (Massachusetts Institute of Technology, November 21, 2002).Bangladesh has many health worries
Over a decade ago, scientists in Bangladesh discovered that drinking water drawn from wells was contaminated with arsenic. The same wells provide the vast majority of the water which farmers use for irrigation. Now researchers have discovered that the arsenic is being absorbed by several crop plants. In rice, they have found high levels of arsenic in the stems of plants, though not in the grains.
Massive problem
Root vegetables are also contaminated. The scientists describe their findings as "preliminary" and stress that many questions remain to be answered. These include the impact on human health and over what area crops are affected. Another concern is that arsenic could reduce the yield of rice, even if it does not enter the grains which are used for food.
Even a cup of tea could be unsafe
While this research goes on, the scientists urge farmers to use surface water rather than wells if possible. The contamination of groundwater in Bangladesh and West Bengal is the biggest mass poisoning in history. The latest estimates are that around 20m people drink water with dangerously high levels of arsenic. More than 10,000 people are known to have arsenic-related diseases, but it is thought that many more cases have gone unreported (By the BBC's science correspondent Richard Black ,Wednesday, 16 January, 2002, 15:23 GMT )
New report again highlights dangerous arsenic levels in Assam’s groundwater
A recently released report draws attention to growing levels of arsenic pollution in Karimganj district, Assam, and the plight of the people who suffer the consequences The amount of arsenic detected in groundwater samples in Karimganj is 10 times higher than the all-India limit of 0.05 milligrams per litre (mg/l) says ‘Preliminary report on groundwater contamination in Assam: Latest findings in the Ganga-Meghna-Brahmaputra plain’, a report released by the School of Environmental Studies (SOES), Jadavpur University, in Kolkata.
Water from 56 villages in Karimganj and Dhemaji districts was analysed by a team of researchers headed by India’s leading arsenic researcher Dr Dipankar Chakraborty from Jadavpur University. The preliminary results reveal that 19.1% of the water tested from 241 tubewells in the region had more than 50 mg/l of arsenic in it; 42.3% had more than 10 mg/l. This suggests that the groundwater contains arsenic elements much beyond the permissible level of 0.01 mg/l, as recommended by the World Health Organisation, posing serious health risks. The report brings to light the fact that around 236,302 impoverished villagers in Karimganj district suffer serious skin and kidney ailments. “Out of the 20-50 children I get daily from many villages in southern and northern Karimganj, at least 25 suffer from hair, nail and skin problems,” says skin specialist Dr N Chakraborty.
The first visible symptoms of arsenic poisoning are dark spots on the skin known as skin lesions or melanosis, dark and light spots, or leuco-melanosis, followed by localised thickening of the skin and the formation of wart-like painful growths or keratosis, ulcers, gangrene and skin cancer. Over a long period of time, drinking arsenic-contaminated water causes skin, lung, liver, kidney and bladder cancers. “We have been drinking this tubewell water since the past five years. Only now we discovered that the water here has the highest concentration of arsenic in Assam -- 444 mg/l. We don’t know what to do now as there are no alternative sources of drinking water in our locality,” says Anulal Das of Kayasthagram village in northern Karimganj. Every member of his family of three is pockmarked with ‘raindrop pigmentation’ (the development of sporadic black and white patches on the back and chest).
The team had earlier carried out water analysis of 1,35,000 samples in West Bengal and 55,556 samples in Bangladesh. The analysis revealed that about 60 million people were drinking arsenic-polluted water beyond the WHO recommended value, while 30 million people were consuming water with high arsenic contamination above 505 mg/l. This placed entire populations at risk. The villagers are now preparing to file a public interest litigation against the Karimganj public health engineer (PHE) in Assam’s Guwahati High Court for failing to take adequate measures to stop the mass poisoning (Source: The Statesman, June 26, 2004)81 pc Bhanga, Faridpur HTW's (Hand tube Wells) arsenic affected,
FARIDPUR, June 8, 2003:–A day-long workshop on "Community based arsenic mitigation action research project" jointly organised by Faridpur District Administration and Department of Public Health Engineering in collaboration with UNICEF was held on Wednesday at Faridpur Zila Parishad conference hall, reports BSS. The workshop was organised to review the progress of arsenic mitigation activities in Bhanga Upazila of this district where arsenic problem is very much alarming. According to workshop sources, in Bhanga 91 per cent Hand Tubewell (HTW) is arsenic affected. Out of 21300 HTW, 19127 HTW are arsenic affected and its water consists very high rate of arsenic beyond human consumption (BSS, 2003).
Smedley, P. L. and Kinniburgh (British Geological Survey, 2002) describes:
The scale of the problem in terms of population exposed to high arsenic concentrations is greatest in Bengal Basin with more than 40 million people drinking water containing 'excessive' arsenic.
"There is a serious concern," says Han Heijnen, a spokesman for the World Bank, "if we don´t take action now, in five to 10 years we will see a very strong increase of the number of people affected either by skin lesions due to arsenicosis or by cancers and other serious conditions. That will be a very serious problem for the socio-economic system of Bangladesh as well as for the health system."
Among 64 districts of Bangladesh, 44 districts have arsenic contamination in groundwater (Mitul, 1998). There are reports of deaths and serious infection relating to arsenic poisoning. It is reasonable to believe that widespread areas of Bangladesh have been contaminated. Arsenic poisoning leading eventually to death,. as world-wide poisoning outbreaks are shown as follows (Pearce, 1995, Chakroborti, 1997):
It is difficult to predict how many Bangladeshis will eventually die from causes related to the arsenic. Most researchers, including Dr. Smith, are shy with estimates. Richard Wilson, a Harvard physicist who is an expert in risk analysis, puts the number at one million. Dr. Sk. Ahktar Ahmad, a public health specialist with the government, predicts a total of three million to five million (New York Times (14. 07. 02).
Chronic Effects of Arsenic (professor Wilson, Havard University, 1999::
- After a letency of 10 years, skin cancers appear.
- After a latency of 29-30 years, internal cancers - particularly bladder and lung. These all have been seen in Taiwan and in Chilie
- The number of cancers expected in bangladesh from the exposure already undergone can be very roughly estimated by using "defalut" (lower exposure of 0. 05 ppm (Bangladesh standard) - the risk 1 %) there are 20,000, 000 to 70, 000, 000 exposed persons at levels between 0. 05 ppm and 0.5 ppm.
India, West Bengal
Arsenic in groundwater above the WHO maximum permissible limit of 0.05 mg l -1 has been found in six districts of West Bengal covering an area of 34 000 km2 with a population of 30 million. At present, 37 administrative blocks by the side of the River Ganga and adjoining areas are affected. Areas affected by arsenic contamination in ground-water are all located in the upper delta plain, and are mostly in the abandoned meander belt. More than 800 000 people from 312 villages/wards are drinking arsenic contaminated water and amongst them at least 175 000 people show arsenical skin lesions. Thousands of tube-well water in these six districts have been analysed for arsenic species. Hair, nails, scales, urine, liver tissue analyses show elevated concentrations of arsenic in people drinking arsenic-contaminated water for a longer period. The source of the arsenic is geological. Bore-hole sediment analyses show high arsenic concentrations in only few soil layers which is found to be associated with iron-pyrites.
Various social problems arise due to arsenical skin lesions in these districts. Malnutrition, poor socio-economic conditions, illiteracy, food habits and intake of arsenic-contaminated water for many years have aggravated the arsenic toxicity. In all these districts, major water demands are met from groundwater and the geochemical reaction, caused by high withdrawal of water may be the cause of arsenic leaching from the source. If alternative water resources are not utilised, a good percentage of the 30 million people of these six districts may suffer from arsenic toxicity in the near future (Source, D. Das et al. 1997)
Country Number affected Taiwan 20 000 Inner Mongolia 50 000 Obuasi Ghana Unknown Cordoba Argentina 10 000 Antofagasta Chile 20 000 Lagunera Mexico 20 000 Cornwall Britain Effect unknown W. Bengal, India 38, 000 000 Bangladesh 50, 000 000
Arsenicosis In Bangladesh : Samta
THE CURSE
This is the story of Samta, a sleepy village in south-western Bangladesh- calm and quiet, and full of traditional natural beauty. A small river called Betna is flowing beside the village which is not extraordinary in nature, but has some certain reasons to be different from others
Now, nobody wants to marry any girl of Samta, nobody wants to choose bridegroom from the village. The reason is that arsenic was found in the groundwater of the village at alarming level. Water of 97% tube-wells of the village is unsuitable for drinking due to arsenic contamination
THE FINDINGS
Symptoms of diseases caused by arsenic have been found in the bodies of 97% people. 16 people already died from arsenic-related diseases and some others are making their journey towards inevitable death. The people of Samta do not know to what extent they are responsible for the disaster or for which reasons they have become isolated from others and are deprived of the sympathies of their neighbours who preferred to keep themselves away from them.
The village Samta is in Sharsha thana of Jessore district. Some 4,841 people live in Samta, in an area of 3.2 square kilometer. Dhaka Community Hospital carried out a survey and tested the water of 265 tube-wells out of the total 279 of the village. It was found that only 2% or 5 tube-wells are safe from arsenic contamination. Arsenic upto the maximum permissible limit was found in the water of 7% or 18 tube-wells while the water of the rest 91% or 242 tube-wells were found totally unsuitable for drinking
Besides, Miazaki University of Japan, the Japan-based Asia Arsenic Network, and Bangladesh Institute of Preventive and Social Medicine also carried out survey at Samta. According to their statistics, there are 284 tube-wells in the village and only 10 of them are safe. Arsenic upto the maximum permissible level was found in the water of 13 tube-wells while the rest 92% or 261 tube-wells were found contaminated alarmingly.
Ten years back, nobody in the village could understand the reasons behind the strange diseases which affected their skins, eyes, lungs, stomach, and intestines. When they found that their skin was pigmented and ulcerated, they thought that it might be leprosy. Some of them thought that these were symptoms of cancer. But the real reason of the diseases was detected in January,1997 when a team of experts led by Dr. Dipankar Chakraborty, carried out a study at the village. They found at least 330 people infected with skin diseases and identified arsenic pollution as the main reason behind it. They apprehended that the number of affected people is higher than the number detected
While conducting preliminary survey, they collected the samples of hair, nails and urine of 334 people and found 99 people affected with arsenic-related skin diseases. The skins of 120 people were not found affected by arsenic. Some 88 children were found affected with skin diseases caused by arsenic while 27 were found safe
But a dpicture revealed when the samples were tested in the laboratory. The presence of arsenic at dangerous level was found in the urine of 324 people (97%), in the hair of 284 people (85%) and in the nails of 321 people(96%), out of the total 334.
Later Dhaka Community Hospital collected urine samples from 301 more people including children. 118 of them were suffering from skin problems caused by arsenic. The results of the laboratory tests of these samples were more disastrous. Arsenic was found at safe level in the urine of only 8 people (3%) while the presence of arsenic at dangerous level was found in the urine of the rest 293 people(97%). After completion of the study, the report apprehended that most people of the village were affected with arsenic. As a matter of fact, a good number of people of this village have died of arsenic pollution. Dhaka Community Hospital has records of their names, age and other particulars (Dhaka Community Hospital, June 2001).
There are hundreds or thousands of such villages in Bangladesh that are not yet known but confronting the worst scenerio like Samta village.
Where it all began
Shahid Alam delves into a malaiseSamta: Arsenic Dushone Akranto Ekti Gram, Daily Star, July 20,2014
JUST a few years ago, the Bangladesh (and several international) media were awash with the news of several parts of the country being afflicted by a variety of illnesses brought about, totally or partially, by the drinking of arsenic-rich water. Then, as other news began to dominate the headlines of newspapers and TV channels, and also probably because the dire situation related to arsenic poisoning had improved enough, the news was relegated to the inside pages, and, that, too, on the rare occasion. If the scenario has indeed become significantly better, then that credit belongs primarily to the heroic efforts of a relatively small number of caregivers, both local and international (specifically, Japanese), who have dedicated themselves to tackling a very serious problem. Samta: Arsenic Dushone Akranto Ekti Gram has been written by one of those caregivers, Manjuara Parvin, detailing her own involvement in the programme run by the Japan-based NGO Asia Arsenic Network (AAN), which focuses solely on arsenic-related problems.
AAN started working in Bangladesh in 1997, and Parvin joined the organization at the very beginning as an everyday worker. Through this association she got to learn about, in her words, the illness called 'arsenicosis', which originates from drinking arsenic-rich water, come in close contact with people suffering from it, and the opportunity to take care of them. She was born and raised in Samta, a village of Jessore, a number of whose inhabitants had been afflicted with the disease (even she had shown early symptoms, but had been cured), and whose story was carried in the print media in early 1996. The news came to the attention of the National Institute of Preventive and Social Medicine (NIPSOM), whose officials visited the village in September 1996 (although, in the Preface, she states that NIPSOM became interested in the then unknown disease --- in Bangladesh --- called arsenicosis in December 1996). AAN then got in touch with NIPSOM, visited various localities of Bangladesh that had been affected by the disease, and eventually settled on Samta, with NIPSOM's concurrence, as the place to center its activities of research relating to underwater arsenic contamination, health issues, and treatment of arsenic-related diseases.
Parvin devotes the entire first chapter on giving an account of her village and her family. Parts of it are anecdotal, others recounted from personal experience, and a few are endearing (maybe even enduring for at least some time to come) folklores. Some of the stories deal with the supernatural, which had happened in her village as told by villagers and her elderly family members, and, at least on a couple of occasions, from her own personal encounters. They will strain the skeptic's credulity, while feeding the flight of fancy of the imaginative, sensitive, or romantic minds. Her multiple encounters with poisonous snakes attest to her sagacity and quick reaction in dealing with them. The village was once, when the British raj was still prevailing in India, under the tyrannical dominance of two Hindu zamindars from the same family, who, even though they liked Parvin's father because he had designed the main door of their mansion, did not fail to mistreat him. They went over to India following partition by the raj.
One of the striking features of the first chapter is the contrast it presents between the way of life and living conditions in Samta before the mid-1990s, and after, an account that reflects the story of the Bangladeshi society in general. While the differences can be measured in terms of the ushering in of the age of globalization and its principal catalyst, the Internet, they can also be viewed in terms of relative prosperity. Parvin talks in sketchy detail about agriculture, food habit, modes of attire, education, the use of television and shallow tubewells in Samta, and shows how much the lifestyle of the villagers has improved from the time when the age of globalization and the Internet had not yet established its foothold on the village. In this section Parvin evinces the ability of not only being observant about the marked changes that had taken place in the village, but also about the preferences of the audiences of TV shows. For example, the viewers in the village prefer to watch the foreign (read: Indian) channels over the Bangladeshi ones. The females like to watch Poshchimbanga and Indian (read: Hindi) drama serials more than anything else.
Particularly interesting in the context of her topic is the section on shallow tubewells. Before the 1970s, the inhabitants of Samta had no knowledge of the use of shallow tubewell water for cooking and drinking purposes. They used the water from ponds, rivers and rivulets, and wells. As a result, they often used to fall victims of water-borne diseases like cholera, diarrhea, dysentery, and typhoid. Since there was a dearth of qualified doctors, the afflicted villagers went to the lone homeopath who prescribed herbal medicines. Mortality rate was fairly high, and gradually people learnt about the water-borne diseases and their origins. Eventually, they had shallow tubewells dug in almost every family home and used the water pumped out of them. Ironically, in Samta (as in several other places across the country), a new disease, directly linked to arsenic that was mixed in the water coming out of the tubewells, was proving to be more deadly than the other water-borne diseases. The upshot of the appearance of the disease and the knowledge of the carrier was for the villagers to go back to the 1970s and the centuries-old practice before that! They have gone back to the ponds, rivers, rivulets, canals, and wells for water to drink and cook in. They have come full cycle and gone back to the past, or is it the future? Learning from past experience, the villagers now purify the water by using filter, boiling, or using bleaching powder. The author is, nonetheless, apprehensive that even in water from deep tubewells, arsenic would be found. Then, she contends, water (purified) from ponds and rivers would be the only safe means for drinking and cooking.
Parvin talks extensively and lovingly about the expatriate Japanese and Bangladeshi doctors of AAN who had given so much of their time and effort to combat the arsenic-related diseases, and to look after those who had been afflicted with them. Among several of these caregivers, the names of Kaguyuki Kawahara, Dr. Sk. Akhtar Ahmed, Sachie Tsushima, Hiroshi Yokota, and Dr. M.H. Faruqee stand out. She extols the Japanese photographer Jin San, who used to help out the families of arsenic-stricken patients with money, something that the affluent of Samta did not do. In a different context, she makes another telling point. In 1997 she was elected a Union Parishad member, and, in that capacity, had proposed that funding be made available for the construction of a paved road from Jamtola Bazaar to Samta Bazaar. She was told that she could have her wish on payment of Taka 40,000 to the local Member of Parliament. She was so mortified that she vowed never to run for public office again. Parvin is convinced that people in Bangladesh run for public office for their individual and party's benefit. They do not much care for the general populace's welfare.
However, the author has her own personal moment of success when, in Japan in 1998, as a participant in the 3rd Forum on Arsenic Contamination of Ground Water in Asia, she succeeded in getting her proposals accepted on establishing an arsenic center in her locality for the treatment and service of patients, and for them to receive medicine free of cost each month. The author noted the similarity in Samta's experience with that of the Japanese village Toroku, whose people had also had suffered from arsenic-related diseases. She observes with satisfaction how AAN's project had been expanded to include Dhaka, Jessore, and Sharsha upazilla. She is pleased that, in a traditional society where almost any change is hard to come by, the villagers have agreed that, more than agriculture and pisciculture, uncontaminated drinking water is of greater signifance. Manjuara Parvin has not written a book that will shake the academics or the movers and shakers of the country. It is a story of a person who has been involved with tackling a deadly disease that has affected a good number of people in different parts of Bangladesh, including her own village of Samta. But she writes with feeling and resolve, and this book is as much a story of her own triumph over adversity as it is of a concerted effort at defeating a deadly disease. One can do worse than going through Samta: Arsenic Dushone Akranto Ekti Gram.
Reported 100,000 cases of arsenic skin lesions: Bangladesh faces outbreaks of cancer (WHO)
Arsenic is a classic poison with a broad spectrum of effects. Unfortunately, although the World Health Organisation (WHO) acknowledged early that arsenic in the groundwater of Bangladesh is a “Major Public Health Issue” which should be dealt with on an “Emergency Basis,” the global community has been slow to respond to the problem of arsenic exposure in Bangladesh, despite the enormity of the problem. But as arsenic is toxic to both respiratory tract and myocardium, long term exposure to arsenic can have erious effects on health and if left untreated, can lead to death.
Far less known is its neurological consequences on people both young and old. However a study of 12,000 residents of Araihazar, Bangladesh threw some light on this aspect that indicated how exposure to arsenic from drinking water was, in relation to the quantity of arsenic found in the water, associated with reduced intellectual function. This study reported a strong association between arsenic exposure and intelligence that is important and tragic, and adds urgency to the need for effective remediation. In addition to the elevated arsenic concentrations found in Bangladesh groundwater, the British Geological Survey reported in 2001 that many of the existing wells in Bangladesh also have manganese concentrations exceeding the WHO standard of 500 µg/l. This is of concern as occupational manganese exposure has been associated with neurologic sequelae in adults, specifically Parkinsonism.
According to WHO, there are at least 100,000 cases of skin lesions in the country caused by arsenic and in addition, the country has to brace itself for probable outbreaks of cancer over the coming decade as the dose of arsenic increases in positive progression for each individual. Estimates now suggest that, by then, one in every ten cases of cancer will be caused by arsenic. That is not a pretty picture, especially as, according to doctors, those suffering from arsenic poisoning are not receiving the care and attention they deserve. That being the case, it is high time the complexity of the situation is recognised and given the priority it deserves.
The human body excretes arsenic at a rate that depends on the individual but if arsenic is ingested at a rate greater than can be excreted by the kidneys, it builds up in liver, spleen and blood. However, if it can be excluded from the diet, this build-up, with the exception of the portion sequestered in nails and hair, will be excreted within days or weeks. But few are lucky enough to look forward to an arsenic free diet because too many people are still drinking contaminated ground water. This worry is intensified by the fact that 63 per cent of tube-wells are contaminated with unacceptable concentrations of arsenic. But the possibility of arsenic poisoning is the most challenging of all the health problems facing the nation for one simple reason, no one can be sure where it will strike, or when, as it takes between 2 and 20 years for symptoms to emerge. And worse - without any external manifestation of arsenic poisoning, a person can still succumb to its consequences either in the form of cancer or due to acute renal failure. Empirical evidence suggests that some stages of arsenicosis such as Melanosis, are reversible, provided the consumption of contaminated water is stopped. In other words drinking arsenic free water can stymie the deterioration of the patient. But as unfortunately no data related to total recovery has been recorded, this statement cannot be supported with statistics. However this does not detract from the major challenge facing the nation - how to provide millions of people with arsenic free, bacteria free as well as chemically safe, aesthetically acceptable alternative source/s of drinking water. Unless an effective action plan on Health and the Environment is put in place, one that can identify the areas of concern and define all possible solutions, the country is likely to be swamped by this crisis because the average person’s understanding of what is called “the largest mass arsenic-poisoning case the world has ever seen” is not only limited but generally erroneous. As such, arsenic poisoning will continue to take its toll on the people of Bangladesh.
Many people have lost a limb to amputation but under the current programme for screening patients, no provision has been made for surgical intervention, nor is there a plan for rehabilitation. Although the Dhaka Community Hospital Trust is doing a good job, their resources are limited. However, DCH doctors have gone out into the field to train Government and NGO health workers in an effort to improve identification and treatment of cases of arsenic-poisoning as patients with severe acute gastrointestinal signs and symptoms may pose a diagnostic challenge. However ingestion of arsenic is the most common cause of poisoning and in consideration of this, diagnosis is essential, because acute arsenic poisoning can be fatal if it remains undetected.
Acute respiratory failure can occur due to severe weakness of the respiratory muscles. Bronchial pneumonia and upper respiratory tract inflammation commonly develop. Central nervous system changes are found, including sudden altered mental status, seizures, toxic delirium and encephalopathic Numbness and tingling of the hands and feet are quite common. Patients may develop an unusual posturing of the hands, brought about by intense dysesthesias in the hands and feet. Severe peripheral neuropathy following several days of exposure to arsenic has also been noted. Dermatologic findings include flushing of the skin, hyperpigmentation and brawny desquamation, as well as dermatitis and folliculitis. Hyperkeratosis, especially of the palms and soles, has been described. White transverse bands across the fingernails and toenails may be observed four to six weeks after exposure.
Diagnosis of acute arsenic intoxication should be considered in any patient with gastrointestinal complaints as the hallmark, including epigastric burning, esophageal pain, colicky abdominal pain, and persistent vomiting and diarrhea, which may be bloody. The vomiting and diarrhea frequently manifest as profound dehydration, leading to cardiovascular collapse and possible seizures (Sylvia Mortoza, The Bangladesh Observer, March 21, 2005)Arsenic contamination severe in Nalitabari
SHERPUR: Arsenic contamination of underground water has become severe in all the villages under 11 unions in Nalitabari upazila of Sherpur district.
Some 15,000 tube wells have been tested in Nalitabari upazila where arsenic was detected in more than 6,000 tube wells, said Water Test Proof sources. A further 10,000 tube wells is under process of examination, they said. A total of 81 men, women and children are now suffering from diseases caused by arsenic. Of them, 17 patients are found in Nalitabari Sadar union, which is the most vulnerable of all. Sources said that presence of arsenic was also detected in water of a total of 88 tube wells out of 148 in Nalitabari Sadar union of the district.The arsenic infected patients are demanding safe pure drinking water, nutritious food and proper medical facilities.
A human chain was formed in front of the Shaheed Minar in Nalitabari upazila town of the district on May 29. The human chain was organised, by World Arsenic Mitigation Committee in collaboration with Caritas, Mymensingh. After the event, the arsenic infected patients submitted a memorandum containing 12 demands to the Nalitabari UNO, said Abu Jafor Babo, president of Arsenic Affected Patients Association.
Caritas monitoring Officer Klodia Nokrek Keya said Caritas Mymensingh has been working to raise public awareness about arsenic contamination in Nalitabari upazila of the district for a long time (The Independent, 05 June 2014 ).
Arsenic warning on 'sacred' water
Water said to be from a sacred Muslim well has been taken off shop shelves, for containing high levels of arsenic. A complaint was made that bottles said to be Natural Zam Zam Water were on sale in central London. It should only be sold in Saudi Arabia. Analysis showed the water had high levels of nitrate and three times the permitted levels of arsenic.
No other shops were found selling the product, but Westminster Council's investigation led to a national recall. Trading standards officers in Barnsley, South Yorkshire, have also received complaints from Muslims about the product being sold.Results 'a shock'
The investigation in Westminster began with a complaint that the water was being sold in London. But the results of a sample sent to the public analyst came as a shock, a council spokesman said. The Food Standards Agency (FSA) said the arsenic "could contribute to increasing people's risk of cancer". There have not been any reports of anyone being taken ill after drinking the water, and no other samples were found for sale. Council staff also contacted the importers to stop them bringing more of the water in.
The FSA has warned shoppers to be alert and report any incidences of Zam Zam water for sale to their local authority - particularly as demand increases during Ramadan.
"This advice does not relate to the genuine Zam Zam water being brought into UK by returning pilgrims... as a personal import," a spokesman said. "As genuine Zam Zam water cannot be legally exported from Saudi Arabia for commercial sale, any product found in the shops would have an uncertain provenance and pose a possible safety risk" ,(Source: BBC, 21 Oct 2005).
Exposure to arsenic could double risk of pneumonia in children under 5 years
In the first study of its kind, icddr,b scientists and international collaborators have found that children under 5 years of age exposed to arsenic had a two-times higher odds of developing pneumonia than children not exposed. The scientists looked at arsenic concentration in urine samples of 153 children aged between 1 month to 5 years with severe and very severe pneumonia.
For comparison, they also looked at 296 healthy children in the same age group. The association of arsenic with pneumonia was present even after the researchers accounted for other risk factors, like weight for height and age.
The case control study was conducted during January 2012 to September 2013 in icddr,b's rural field site Matlab with colleagues from Mailman School of Public Health at Columbia University, USA, and Johns Hopkins Bloomberg School of Public Health, USA.
Pneumonia is the leading infectious cause of death in children worldwide, accounting for 15% of all deaths of children under 5 years of age.
In 2013 alone, an estimated 935,000 children under the age of five died of pneumonia globally. In Bangladesh, the biggest cause of death for children under 5 years of age is pneumonia, accounting for 27% of all deaths. Worse, it is estimated that more than 35 million people in Bangladesh are at risk of being exposed to arsenic concentrations that are greater than the national standard and the World Health Organization guidelines.
Dr Christine Marie George, lead author and assistant professor in the department of international health at Johns Hopkins Bloomberg School of Public Health, said the findings suggest that "even low to moderate arsenic exposure may make children more vulnerable to pneumonia. This is likely because the arsenic in their drinking water is weakening their immune systems, making them more vulnerable to infections."
Senior consultant on the study and former head of icddr,b's Matlab Hospital Dr Mohammad Yunus said chronic arsenic exposure reduces CD4 T cell numbers, which are vital for mediating adaptive immunity to a variety of pathogens, affecting the overall immune functions of the human body.
This could increase risk of pneumonia in children (The Daily Observer,Friday, 6 November, 2015).There are major differences in institutional arrangements in the two countries. Bangla- desh has a highly developed and effective NGO sector, and the goverment has welcomed foreign assistance.
Differences between West Bengal and Bangladesh
West Bengal, being a ‘communist’ state, favors government intervention, and is less amenable to foreign assistance.
For instance, both UNICEF and the World Bank are playing leading roles in arsenic mitigation in Bangladesh, but are doing relatively little in West Bengal. In Bangladesh, NGO projects currently cover about 75 per cent of villages, reaching a quarter of the population, and attracting more than US$ 500 million annually from foreign donors (Haq, 1997 in Hossain et al., 1999).
The existence of these extensive NGO networks, and their close links with donors, has helped raise arsenic awareness and expand mitigation efforts more rapidly than has been possible in West Bengal.
More than 9,500 field test kits have already been sold in Bangladesh (of which 90 per cent have been Merck kits), and more than 200,000 arsenic ests have been completed using field test kits. In May 2000, another 8,000 Merck kits were ordered by BAMWSP, and tenders for a further 50,000 kits are currently being evaluated. In contrast, sales of field test kits in West Bengal total only about 1,000 kits. The figures for Bangladesh look more impressive, but conceal the fact that both countries have only provided arsenic removal units to about one per cent of the affected household
Another difference has been in the role of the private sector. In Bangladesh, the government owns 92 per cent of modern industries and privatization efforts have been relatively slow (Hossain et al., 1999). BAMWSP is coordinating closely with the NGO sector, and most stakeholders are waiting for BAMWSP to validate technologies before they consider large-scale implementation. Local manufacturers have limited research and development budgets, and are waiting to see which technologies are going to be validated before investing in production. Thus,innovation and experimentation by the private sector are being stifled.
In West Bengal, there has been little coordination of arsenic mitigation efforts, and it appears that many in government favor the provision of alternative water sources over arsenic removal units. Despite this, there is evidence of genuine private sector participation, albeit at quite a small scale. Oxide (India) have developed and refined their own arsenic removal unit, built a network of seven dealers, made more than 500 private sales, and are actively engaged in marketing, including printing 5,000 leaflets for distribution through their dealers, and running a stall at a trade fair run by the Bengal Chamber of Commerce.
There are also three local manufacturers involved in the production of field test kits. It has been suggested that longer awareness of arsenic contamination in West Bengal has contributed to this higher private sector participation, but there is little evidence to support this, and it seems likely that any differences have been created by the dissimilar institutional arrangements.
Field test kits provide an example of technology difference. The imported Merck field test kit has become standard in Bangladesh, but has not been very successful in West Bengal, where AAN type field test kits are preferred. There are several possible explanations for this difference. Firstly, the smaller scale and seriousness of the arsenic crisis in West Bengal has combined with lower ESA involvement to result in less scrutiny of field kit performance than in Bangladesh. Secondly, local reagents and raw materials are cheap and freely available in India, while import duties are high (Merck kits are more expen- sive in India than in Bangladesh).
Finally, anecdotal evidence suggests that groundwater sulfide levels are generally higher in India, so field test kits without a sulfide removal stage, such as the Merck kit, are less effective.
Another striking difference is in the adoption of arsenic removal units using adsorptive media. There have been a number of field trials in Bangladesh, but few of them have been successful and there was no evidence of the adoption of adsorption units on a larger scale. In India, sales of the Amal filter are growing, and there are several community handpump units operating successfully. Again, there are several possible explanations. Most of the successful adsorption installations are based on activated alumina, which is manufactured in India, whereas manufacturers in Bangladesh have to import the media, and are hindered by import duties and bureaucratic delays. Another factor may be the aquatic chemistry. The areas of Bangladesh visited during this study had exceptionally high levels of iron in the groundwater, which created severe clogging in any sort of filtration unit, and severely limited the viability of single stage adsorption units (Arsenic Mitigation in West Bengal and Bangladesh Helping households respond to a water quality crisis, December 2000).Arsenic Contamination in Drinking Water in India
The danger of arsenic, a fatal metalloid contaminating the water reserves in the entire world is on the rise. The metalloid has poisoned about 140 million people though out the world and has the highest toll in developing countries such as India. The risk has found existence from large-scale tube well drinking water facility initiated in the 20th century. The water program started with the aim of protecting surface water against the bacterial contamination found in high levels. The research done did not pay attention to the fact that arsenic; a soil ingredient leaches into the underground water resulting in vast population effected by the deadly contaminated water mostly in Vietnam, Cambodia and China. The population in North America saved through the utilities that purified this water.
The rice cultivation in such areas affected due to high level of arsenic found in the irrigation water. Nearly a majority of population in South and East Asia is exposed to high arsenic poisoning. Arsenic found in pesticides and insecticides also used as wood preservative and for combustion of fossil fuels. Contaminated drinking water forms the base of arsenic poisoning in the human body. Tumor in lungs, skin, kidney and urinary bladder are the result of Arsenic infection. Cancer and skin problems observed in people exposed to arsenic infection found in 0.05mg/L drinking water. The starting effects occur on the skin that worsens to caner conditions. Cardiovascular diseases, diabetes and reproductive disorders are some of health problems that occur due to high-level arsenic poisoning in drinking water.
Arsenic contamination can lead to a number of problems depending upon the effect on the potassium in the body. High level of Arsenic in drinking water held responsible for hypertension, erectile dysfunction, diabetes, depression, obesity and other conditions leading to alteration of intercellular potassium volume. Long exposure and intake of arsenic infected water has irreversible effects on people. People working in industries have high chances of infected with arsenic leading to premature death and long-term illness. Farmers using pesticides and insecticides have high chances of arsenic exposure. Mining workers often accumulate high level of arsenic in their respiratory systems leading to liver cancer, lung cancer.
In India, the first case of arsenic contamination came in West Bengal during 80's when tube wells held responsible for the contamination. The wells were having depth between 20-150 meters. According to Dipankar Chakraborty, head of school of environment studies in Jadavpur universities the situation started by arsenic polluted drinking water in eastern India was of alarming rate. More than 1000 villages in West Bengal infected with arsenic contaminated drinking water. Chakraborty and his team adopted measures to control the amount of arsenic contamination in water such as
Thirty five percent of villages in West Bengal have tub wells with safe drinking water, and tested every 3-6 months. Epidemiological research is required to know the arsenic contaminated areas to know the health hazard and report the benefits in exposure of arsenic.
People made aware about the danger of arsenic infected drinking water. Arsenic contamination in drinking water reserves both in India and Bangladesh has reached critical levels and needs to be tackled before the situation gets out of control. (Article Source: Jaceline_Peirrera)Arsenic patients increase in Kushtia
KUSHTIA, Dec 22, 2014, Daily Observer: The number of patients attacked with arsenic-related diseases is increasing alarmingly in different parts of the district. It is alleged that due to lack of regular visit of the field workers of the Health Department, the number of patients is increasing unabatedly.
Sources at Kumarkhali Upazila Health Complex said that the number of arsenic-affected patients in the upazila was 242 last year. But the number has increased rapidly with 412 patients this year. It is also alleged that the trained women workers of the upazila health complex had done nothing to detect the arsenic affected patients in the upazila. As a result, the situation has turned worse. The arsenic affected tube-wells were detected marking red signs and the users were asked not to use the water of the tube-wells marked in the year of 2001 in the district for the last time. The red-marked tube-wells were identified for not to drink and use the water. Dr Akuluddin of Kumarkhali Health Complex said that the green marked tube-wells might have already turned into arsenic affected ones. He also said that most of the arsenic free tube-wells installed by the government have already gone out of order due to lack of proper maintenance and monitoring.
According to him, there has been a project for setting up new arsenic free tube-wells under Kumarkhali Upazila Public Health Office. But the office has not yet showed any interest to repair the old ones for using. Sources in Public Health Office of Kumarkhali upazila said that 30 per cent water in the newly set up tube-wells has been contaminated. As a result, the inhabitants of Kumarkhali are very much worried about the health hazards caused by arsenic.
The menace of arsenic is coming rapidly as the level of the groundwater is going down very rapidly. Scarcity of pure drinking water has gripped the district as most of the groundwater has been contaminated. It was very easy to get pure drinking water from the underground level ten to 15 years back. Some 16,000 tube-wells have been tested in Daulotpur upazila where arsenic was detected in more than 6,000 tube wells, said Water Test Proof sources. More 10,000 tube wells are under process of examination, they added.
A total of 100 men, women and children are now suffering from diseases caused by arsenic. Of them, 17 patients are found in Daulotpur Sadar union, which is the most vulnerable of all. Sources said that presence of arsenic was also detected in water of a total of 88 tube wells out of 148 in Daulotpur Sadar union of the district. The arsenic-infected patients are demanding safe pure drinking water, nutritious food and proper medical facilities. At present, the people of the district face problems to obtain drinking water as the contamination has been growing quickly day-by-day. Sources said that the level of contamination is very high in the unions of Shelaidah, Jagannathpur and Chandpur of Kumarkhali upazila. The patients of these areas have been suffering a lot from skin diseases and black marks are visible on their bodies.
The inhabitants of Hasimpur and Dayarampur villages under Jagannathpur union said that they feel pain on their chest and backbone. They are absolutely helpless and they do not have any opportunities to prevent the deadly disease. They said that they had been prescribed some medicines in the month of July in the last year. But nobody took any care of them afterwards.
Sajida, Kulsum, Vanu and Fatema are among the villagers who have been attacked with arsenic diseases at Hasimpur village. Kulsum Begum alleged that they are passing their days in panic as no government or non-government organisations have come forward to mitigate their sufferings. According to the Department of Public Health of Kumarkhali, the level of arsenic contamination is very high because they are living beside the river Padma and experts of the office said that the level of contamination rises at very high rate when it is boiled. - See more at: http://www.observerbd.com/2014/12/23/62296.php#sthash.HBkpo3d6.dpuf2929 arsenic patients detected in ComillaPublished : Saturday, 21 March, 2015
COMILLA, Mar 20: The arsenic contamination has been detected in the water of 78.93 per cent tube-wells in eleven out of sixteen upazilas of the district, according to an official source. There are 41,943 tube-wells in 16 upazilas of the district. The Public Health Engineering Department (PHED) conducted a sample survey in the water of 3,029 tube-wells in eleven upazilas of the district, and water of 2,391 tube-wells was found arsenic contaminated, said Executive Engineer Mozaffar Ahmed of Comilla PHED.
According to Comilla Civil Surgeon office, a total of 2929 people have been suffering from arsenic-related diseases, the sources added. Of them, 480 are in Monohorganj upazila, 562 in Laksam, 48 in Homna, 228 in Daudkandi, 724 in Muradnagar, 120 in Dabidwar, 596 in Chandina, 32 in Barura, 13 in Chowddagram, 91 in Nangolkot and 35 in Titas upazila of the district.
The water of tube-wells in Comilla Sadar, Sadar Dakkhin, Burichong, Brahmanpara and Meghna was not affected with arsenic contents, the sources said. In Barura upazila, the PHED conducted the test in the water of 254 tube-wells out of 3,354, in Nangolkot 209 out of 2,420, in Laksam and Monohorgonj 142 out of 4,992, in Dabidwar 210 out of 3,259, in Chandina 208 out of 2,499, in Muradnagar 336 out of 4,582, in Daudkandi and Titas 400 out of 4,964 and in Homna 396 out of 2,619 tube-wells.
An arsenic affected female patient in Eruain village, seeking anonymity, said to avoid social harassment she got treatment at her father's house instead of her husband's house. Another patient Faruk Ahmed at Charbaria village of the same upazila said some NGOs distributed medicine earlier but now they are not doing this. He demanded to set up more arsenic free tube-wells in the area.
Nur Hossain, Kandirpar Union Parishad Chairman under Laksam upazila alleged the Health Department is not giving proper attention to the arsenic affected area. Dr. Md. Salah Uddin, Laksam upazila health officer, said, "There is sufficient stock of medicine in the health complex. If patients demand medicine, we supply it as usual."
During the survey, the PHED put red mark on the arsenic affected tube-wells and advised people of the area not to drink water of the those tube-wells. Though the arsenic contaminated tube-wells were sealed off, people are using water of these tube-wells as there is no other alternative source of drinking water in the affected villages of the district. Comilla Civil Surgeon Dr. Mojibur Rahman, said rain water is free from arsenic contamination.
A survey recorded that ring well popularly known as "Pathkua" is also free from arsenic contamination. According to World Health Organisation (WHO), 0.05 mg arsenic per liter of water is the tolerable limit for Bangladesh. But sample collected from different parts of the district indicated that the high percentage of the arsenic contents like 0.51mg in the tube-well water is extremely dangerous for public health. It may be mentioned here that the test of arsenic contamination in drinking water by the SDC Laboratory of the PHED cost Tk 300 to Tk 500 per tube-well. The government should conduct free tests to detect arsenic contamination in tube-well water for the better interest of (Daily Observer, 21 March, 2015Last Modified November 8, 2015